


"Staying off Empty" Pt. 2
The Case Against Harm-Reduction

“Staying Off Empty” Pt. 2
The Case Against Harm-Reduction
Matthew Kirkus 2024
“Society cannot exist unless a controlling power upon will and appetite be placed somewhere, and the less of it there is within, the more there is without.” Edmund Burke
Harm-reducitonists are chiseling away at our inherent notion that recreational drug use is wrong. What is true and Good should guide policy and what is pragmatic, like harm-reduction, should be guided by the former.
Safe-Supply is enablement, post-modernists are reframing the issue. For them, neither the addict nor the drug abuse is a problem but society is. Drug abusers not only have the right to use but furthermore the right to demand the government provide for their addiction.
“shuttering the clinics that have allowed them to become independent of the illicit drug supply, they argue, violates their right to life, liberty, and security of the personal and the right to not be subjected to cruel and unusual treatment. They further contend that this constitutes discrimination on the basis of physical and mental disability.” OO 253
”access to a treatment that effectively eases pain, both physical and emotion, is a disability right. Not because, as pain patients sometimes say, they have the right to pain relief, but because, like everyone else, we have the right to accommodations that afford us the chance to realize our potential.” OO 261
Throughout this paper you may come across opinions of which you disagree but I lay out the controversies and my opinions clear from the onset. I am not spoon feeding you or protecting your feelings. Beside my own satisfaction I have little to gain by doing this work, it is you who who will gain a deeper understanding of this still-largely unrealized emergency. I understand many don’t read or have patience or perseverance in our instant-distraction filled environment but I propose that if you care about this issue you consider my detailed presentation in full.
It is easy to write a few pages on some of these issues but it is much more daunting and at times upsetting to formulate opinions for every minor detail and present the facts and those opinions in a cohesive manner. It is easy for one to hold opinions on issues they know little about but much more difficult to attempt to understand an issue fully because you will inevitably find yourself in limbo on some particulars. Many leaders will find themselves overwhelmed. Because this issue is only going to get worse I will likely continue my research in this field and because this presentation is so comprehensive this work will not soon be obsolete. I might just as easily choose to stop following this topic at which point the duty is on you to carry on. This paper is a sequel to my previous fentanyl paper https://mattcircus.substack.com/p/money-for-fentanyl as well as writing I have done opposing commercial weed and videos on addiction. https://mattcircus.substack.com/p/commercial-weed-is-dollar-general
I’m sure you can find some reason to personally bash me and my beliefs but I would suggest you remain on topic as this is not about me. Argue ideas.
During a discussion with my Mom she downplayed my efforts to unravel this issue. I discovered about myself that I am not doing this work for street users. I actually don’t have much respect for the majority of these people who don’t work but instead steal, refuse to develop themselves, are only a burden to their community, and may even spread violence. Given few words to sum up our nation I might chose “wasted potential”. I study and develop critical opinions on many issues. I am sickened by this society. I’m not telling you what to do to fix the Fentanyl issue, my purpose is to the expose the woke-agenda piloting harm-reduction. If I aimed to motivate you I would encourage you to find your own issue to fully understand. I spent 8 months on this presentation and it still seems like the minimal needed to begin understanding it.
I prepared many video clips but used very few, perhaps I will make a video presentation or display them during live presentations. Obvious my fragmented use of media falls under fair-use; this generates zero revenue, only aids education, and absolutely bashes recreational drug use. The only criticism of me would be of harboring a different opinion. I would argue than any creators who flag me care less about education and treatment and more about gripping their “virtually” worthless intellectual property. Substack has an issue embedding my many videos so they will have to be presented differently (in another post titled Pt. 2 Media Supplement). I spent just as much time watching and editing video as writing this. I want to wrap this up already but any loose ends in the future will be added to the bottom of Pt 2. 2 Media Supplement.
https://mattcircus.substack.com/p/test-incomplete-staying-off-empty
I wish I could edit it more, I wish I could reread it over again, I wish I had a grammar tool, I wish I had an editor, I wish I was more confident, I wish it was shorter, I wish people would care enough to read it; but I know how it is. I wish I could remove more of my ego. But this is it. To be honest I never spent more time on any specific thing in my life. I just reserached and installed a brand new car engine and the time and energy spent on that is minisccule compared to this. And my time didn’t go to editing either, so be easy on me. Enjoy
I upset Ginny Burton, an abstinence-based advocate; I learned a lesson and admit I was wrong. I will have to paraphrase her position because I don’t have her permission to share her words but I do appreciate her perspective. I respectfully tried to push back from her total-abstinence based platform but don’t believe she is interested in opposing opinions anyway. I endorse her nonetheless and recommend you consider her work. In speaking with her I realized that I will present many opinions of which you (or she) may vehemently disagree. But that’s the nature of free-speech; hopefully you can look past that and find the information that is relevant for your personal journey. (Ginny ep2, 2 clips)
(jaeson .391) The Fentanyl Epidemic: Jaeson Jones & Dr. Michael Jensen on What Must Be Done to Stop It, Real Talk,Published on May 15, 2024
If your prerogative is to blindly accept the consensus narrative then my writing is not for you. If you are easily offended by opposing opinions then this is your trigger warning. I spent a long time preparing this presentation and it covers vast ground. The topic lends itself to video and audio clips which assist in holding the readers attention. Some of the writing is difficult to navigate but so is the topic. This is a long presentation but beyond valuable in understanding where you decide to stand on fentanyl treatment. Please share my writing, especially with anyone in this field or battling addiction; I assure you it is more valuable than most professional content. I would note that I am not perfect, if I made a mistake in my analysis it is an honest mistake, there is a lot to go over. If you are going to read my earlier work keep in mind any mistakes are corrected in this later work. I laid out a large blueprint therefore I am bound to make some kind of mistake. Sorry for any unnecessary repetitions; writing and editing 90 pages on one subtopic by yourself is not too easy.
*
On Opium author Carlyn Zwarenstein spent a majority of her book telling her story as dependent on opioids for her lifelong chronic pain condition; Ankylosing Spondylitis. She uses her love of classical literature to guide the reader through her views on opioids.
“quality of life not having been a major goal of medicine in ages past. Dr. Thomas Dormandy, a pathologist and author, writes that quality of life was an invention of the Romantic age propped up by opium.” OO 48
“The romantic craze started, believed Scottish surgeon Thomas Trotter, with dependence on stimulants like coffee and tea- gateway substances along the slippery cobblestone path to the opium den.” OO 33
I make this same point about nicotine, alcohol, and caffeine as gateway drugs in my previous videos (links at bottom), these studies grant some legitimacy to the brain disease- model of addiction.
Here is the original YouTube information for my claim:Addiction and the Brain- AMNH SciCafe, June 22, 2016, Psychiatrist Edmund Griffin
(this is a very weird .543)
Their is no conventional treatment for stimulant addiction. One solution may be to taper down with legal stimulants. I found this from YouTube channel :The Daily Dose of Mental Health, 12/7/22, Is VYVANCE the SAFEST amphetamine | vyvance vs. adderall | what is amphetamine use disorder?
“One study showed that giving ADHD medication called lisdexamfetamine to patients who are using both opioids and cocaine can help them reduce their cocaine use,” AF 164
*
I am not comfortable disclosing what opioid I was addicted to as a teenager but I was addicted to a novel opioid. I never viewed my early drug of choice as such but it is only fair to the reader and myself to admit I have had a history, no matter how nuanced. When I made the decision to quit I told myself I would return to using when I had my life in order as a kind of retirement. I required that narrative in order to let it go. I didn’t find out it was an opioid until years later. Further regarding my authority on the topic; I am an open kratom user which is very similar to an opiate and can accompany a destructive addiction like other opiates. I have also been homeless and incarcerated for substantial periods of time.
If you have never been homeless without familial support or so fried on pills you can’t string together sentences then you cannot appreciate how homeless addicts feel. I have battled and overcame many addictions and despite popular opinion; alcohol, cigarettes, and marijuana are very addictive.
“In fact, nicotine is nearly as addictive as both heron and cocaine.” AF 20
or that is another lie; (Dr. Ardis will address this later)

I don’t hesitate to declare my pride in conquering these addictions because every day I watch those around me unable to free themselves despite the negative consequences. Most are too near sided to grasp the toll addiction takes on their lives. Instead of admitting the problem and discovering a desire to quit addicts often double-down and defend drug use.
*
I’m not writing an introduction, history, nor legal analysis. I focus on the controversies surrounding treatment which include causes and prevention. I am not merely regurgitating what followers are preaching at the local needle-exchange. I take the controversial position against harm-reduction. I am not financially interested or a status-seeker as are many in academia, nor do I profit from my writings (no paid subscriber option or Chinese made t-shirts). I am merely a laborer so I laugh aloud as I expose the frauds and “intellectuals”. This is real money with real human casualties.
I write for the individual who chooses to free themselves from addiction but I know few if any fentanyl addicts will read this. In case you desire to quit any addiction be prepared to use this information as motivation. Those with wise friends and loving families may not yet be affected by Fentanyl addiction or “harm-reduction” protocols and its accompanying ideology but it will soon creep its way into the nearest restroom and your children's private spaces. If your not finding burnt foil and dirty needles yet you will have clean needles shoved in your face soon enough! It is easy to use hyperbole to criticize the far-left and their harm-reduction “tool-kit” but not as easy to defend a conservative position.
(San Fran regrets its drug policy) San Francisco REGRETS Its Progressive Drug Policies, Published on Jan 11, 2024
(Boofing x2) Hang on! What is "Boofing"? And why are YOU paying for it? | Redacted w Natali and Clayton Morris, Redacted, 6/17/2024
I chose to spend my time on this topic because I think my advocacy can make a difference unlike fighting for my rights in court or voting and pleading with elected officials. This is largely a debate regarding the states role in our private lives. I expect any state action will only worsen the epidemic. I will propose public solutions but I am also a defeatist. My bias does not discount my work. Neither does my lack of experience with severe opioid addiction, in fact I would argue my perspective is more valuable due to my dedication to the topic than any random ignorant street addict. I do agree the patients should have a voice but not to the exclusion of other perspectives. In part 1 I argued against giving recovered addicts any authority recommending they find a new life away from drug issues; relapse is not the exception but the most likely outcome for hard drug users.
I am not emotionally invested as bereaved parents calling for blood. My passion comes from my own history as homeless and addicted. I view harm-reduction advocates as useful-idiots for the woke establishment and hardliner conservatives as equally ignorant. I do not believe harm-reduction solutions are grassroots but designed and promoted to dismantle our remaining culture, liberty, and private ownership. Just as “benevolent” billionaires (Amazon and Ebay) fueled racial hatred during the “mostly peaceful” BLM protests, harm-reduction advocates share the same WHO UNAIDS (the Joint United Nations Programme of HIV/AIDS) agenda, “they recommend a full suite of services for patients who use drugs, including needle exchange programs, opioid substitution therapy, HIV testing and counseling, HIV antiretroviral therapy, prevention and treatment for sexually transmitted infections, condom programs, and treatment for hepatitis and tuberculosis. [Which includes giving] HIV-negative patients antiretrovirals;.. challenges include difficulty of convincing people to take medicine when they are not sick.” AF 150
Instead recently Alaska suffers severe cognitive dissonance while it increases penalties but also allows the tentacles of harm-reduction to take root. Alaska must not understand the goal of harm-reduction is legalization and lifelong drug addicts.
(live alaska .995) LIVE: State leaders address fentanyl drug campaign, Alaska's News Source, 5/7/2024
“Harm reduction” cleverly adopts a facade of grassroots activism. The “left” absolves the guilt of drug users while the “right” wants to persecute indiscriminately.
Meaning, Purpose, and the role of Poverty
Christian treatment centers
While I am a follower of Christ, I will criticize Christian organizations for imposing their beliefs on those in need of charity. I am against this form of blackmail. I am against bible studies or church services before feeding the homeless (especially if receiving state funding). But I am not against prayer that glorifies Christ because it is our culture and a blessing is tolerable whereas bible studies or mandatory services are aggressive and tedious. Despite my conservatism I support secular solutions and “inclusivity” of religions into political and social matters. I believe the best we can hope to salvage of our nations heritage is our legal tradition founded on natural law principles and Reason and not simply Revelation. I don’t believe being aggressive about Christianity will win hearts. This is a great object of debate and my own heroes may disagree but we increasingly live in a pluralistic and secular society in which religious truths are all but impossible to ascertain, as proven by dispensationalism among the christian-right today. Forcing our beliefs onto others is not fair and is not charity. America in large part was founded on Christian/ Greco-Roman thought but with Freemasonic underpinnings; America has always been a contradiction. Is it a mystery why people numb their cognitive dissonance with drug abuse? Don’t confuse our legal system with morality or religion. Certainly our current regime has no moral authority. You are welcome to disagree as this is simply my opinion, I am born and raised in the United States. I had to say this because many drug treatment centers are Christian based and I know before I discovered Christianity for myself (without others forcing it onto me) I did not appreciate their pedagogy. I acknowledge their commitment to their faith but I must insist on this caveat that if the goal is to help addicts as charity then loosening religious dogma is most effective. Of course saving individual souls supersedes physical issues but my argument is that focusing on religious conversion pushes away addicts. I view state programs as totally corrupt leaving only the private charity sector. Worship and discovery is an act which should be engaged in freely and forcing beliefs on someone desperate for help is not charity. A gift (charity) is something given freely with no expectation.
(homeless faith based programs) Homeless faith based programs need to stop pushing so hard for a homeless person to believe in God., truthonthestreets, 6/16/2024
(the faces of Portland) The faces of Portland's now-declared fentanyl state of emergency, The Story, Jan. 30, 2024, KGW News, 1/30/2024
(this is a very weird .050) This Is a Very Weird Moment in the History of Drug Laws, New York Times Podcasts, 5/10/2024
(this is very weird .120)
(this is very weird .036)
“Many detox or treatment centers won’t even accept a referral from a doctor or family member because they want the patient to be motivated, to prove to themselves, and others, that they want to stop using….[but] we make the call because we know their illness makes it impossible for them to act promptly or rationally” 139 AF
(how overdose .882 3) How Overdose Became America’s Silent Killer - With Sam Quinones, The Lonely Podcast, 12/24/2023
Even worse, they become less sensitive to the stimulation for non-drug-related rewards, and they lose motivation to do quotidian and necessary activities such as show up at work and maintain their relationships. AF 18
Family
“80percent of children said their parents were the leading influence in their decision to use alcohol” AF 172
The advice [from Iceland] the importance of giving young people opportunities to pursue “interesting activities to keep them busy, happy, and productive.” AF 173
[Iceland 1990’s] the kids without problems were more likely to be involved in organized sports, spent more time with their parents, felt cared about at school, and were not out late in the evenings.. The government made physical activity for youth easier and cheaper. It created subsidies and encouraged youth to join teams.. teens were either participating in sports or at home with their families. Alcohol use, cannabis use, and smoking all declined dramatically. AF 169
“I believe more strongly than ever that the antidote to heroin is community” San Quinones, Dreamland
Drugs are A solution
“I think that in the popular image of the prescription drug user, the drugs become a numbing substitute for life, but that is the opposite of my experience.” OO65
“Then prime Minister Margaret Thatcher began closing down the coal mines. Until 1980, villages essentially built around mines had experienced only very low rates of unemployment. These were folks who worked hard and lived modestly. In a series of policy measures that now familiar around the world and known collectively as “austerity,” Thatcher imposed deep cuts to social programs and public services, which had a devastating impact on the now out-of-work working class.
Suddenly Buchanan tells me, areas of high deprivation and new unemployment were overrun with teenagers and young adults “off their heads with heroin.
The young people I was working with struggled in school, couldn’t get qualifications. Life was brutal for them and being made more brutal.” They turned, he says, to obliterating their lives. It’s important to understand- especially today, when we hear a lot about “deaths of despair”- that these hopeless people didn’t simply set themselves on fire or slit their wrists. Instead, they made choices that may be seen from the outside as despairing or giving up on life, but which made sense in many ways, given the options available to them.
Heroin and the lifestyle it demands, provided essential things that had otherwise disappeared for young people who had expected to follow a path..as their fathers. before them…Instead a different form of “underground” offered them “employment”- a seven-days-a-week, fifty-two-weeks-a-year job getting and using heroin. Acquiring drugs and paraphernalia to use them involves basic skills like bartering; shoplifting for money to buy drugs involves cunning, clarity, and dexterity.
It gave them identity. It them a purpose. It gave them a reward.” Buchanan recalls. These are all things that people need. In a sense, heroin didn’t just ease pain: it met the set of needs that keep us all emotionally afloat. What Buchanan thinks was missing from his analysis was a real understanding that for his clients, heroin was not the problem: “heroin is the solution”. OO89
“Far from being passive, poor people and people who use drugs actively struggle to improve their lives. We just often misinterpret what we see. Nevertheless, there is despair, plenty of it. And, yes, there are deaths.” OO91
“When bored or alienated teenagers begin using prescription opioids.., this is a solution, for better or for worse, to their boredom and alienation.” OO94
When workers at oil refineries.., or workers in precarious, tough jobs in construction (with little stability or support in the event of an injury) are prescribed a short-term opioid and find that it helps them manage pre-existing chronic pain or deal efficiently with chronic depression, this, too, is a solution.” OO94
“we focus so much on despair that we don’t give drug users.. enough credit for their ingenuity and survival skills. For better or worse, opioids and other mind and mood-altering substances can be expression of both ingenuity and persistence. They can be a practical response to fragmented lives, impossible communication, and chronic lack of support. Not despair, not lack of self-respect, but the desire to feel better, to transcend pain.” OO 96
...“Addictive substances are appetitive and reinforcing,” Skinner says Appetitive, a lovely word, in that such substances satisfy deep appetites for pleasure. And reinforcing, because such pleasure carves strong, memorable grooves into the psyche, particularly in people who for some reason feel they need it. People who are opioid- dependent have higher rates of depression than in the general population. Addiction problems tend to be accompanied by mental health issues” he tells me. It’s not that easy to tease out the direction of causality, but there is reason to believe that people seek out the drugs that help them feel okay. “For example, people with anxiety may find relief in drinking alcohol or smoking pot, while those suffering with ADD may turn to stimulants, including cocaine, to self- medicate their symptoms”. He also mentions that conflict avoidance is an issue for many opioid users.” OO54
Housing First
“a mantle taken up by the housing first movement, which advocates that “all people deserve housing, and that adequate housing is a precondition for recovery.” AF144
Some may propose State funded housing for the homeless because it’s hard to quit drugs while living on the street. While I partially agree I contend our government was not created to redistribute wealth but is intended to defend private ownership. I promote private charity and may even defend “socialism” (such as a right to access the commons and access to the means of production and soil) but am skeptical of abuses inherent in welfare programs. I am also weary of conflating separate issues.
(How the usguil .878 seg 6,seg 7) How can the US solve the Fentanyl crisis? | Sam Quinones, Giuliano Giacaglia, 12/21/2023
(how overdose .765, .710) How Overdose Became America’s Silent Killer - With Sam Quinones, The Lonely Podcast, 12/24/2023
“They may see it this way even though the causal relationship between drug use and outcomes like homelessness is not a simple matter of drug use causing homelessness. In fact, most evidence suggests that drug use and housing precarity often share similar causal factors, such as poverty or, more specifically, low wages or income and high costs.” OO92
“Such a large part of the American population is in this misery situation, in deep debt, one paycheque away from serious housing precarity, it’s almost surprising that drug use and overdose rates are not higher than they are.. Many also use addictive or euphoric or appetitive substances, from prescription and benzodiazepine, to cannabis, to alcohol, to amphetamines. But only a very small proportion become homeless as an apparent result of drug use, and in fact available research shows a relationship between homelessness and substance use that is neither one-way nor direct.” OO92
I intercede to remind readers Fentanyl does not fit the mold of any previous addictions. I imagine it’s abuse is more closely tied to homelessness than previous drugs were. This still doesn’t make it causal but the correlation is stronger. As the general public continues the decline into poverty drug abuse and homelessness will also increase. Yet, for average addicts there is always money for beer, cigarettes, and weed; if you have these addictions you know what I’m talking about! I often point to the coffee and pastry business plan; it doesn’t matter how poor we get, we always find a couple dollars for these quick distractions.
*
I volunteer at a homeless shelter. I talk to seasoned staff about the woes of their clients. We start with cliches like “you can’t help someone who won’t help themselves” but neither Bert nor I are amateurs so our conversations get deep as we whisper while 25 guys fall asleep around us. Bert essentially says most people don’t succeed in the program (which includes life skills, employment, and housing) but instead they live in the shelter for years. They aren’t using the program as a stepping stone but instead simply maintaining their current lifestyle. They often leave in the morning, drink or abuse drugs all day, and come back to sleep at night.
When I began volunteering I was eager to help the less fortunate but it didn’t take long for me to grow cynical. I reconciled the fact that I wouldn't be assisting people better their lives but simply serving there as charity.
The conflict arises from our expectation of them to use the program to become autonomous. If the program were charity alone we might stand aside and give them a place to stay comfortable while they give up and waste away but that's not the intent of the program.
I respond to Bert, I make a comparison to harm-reduction. Harm reduction does not solve anything, it “kicks the can down the road”. It’s charity, not treatment. I was surprised by his response; he told me when he heard about needle exchanges and safe consumption sites he thought it was a ridiculous idea because it assumes that these users aren’t simply going to share needles next time somewhere else.
Maybe these sheltered homeless don’t have hope for their future or for society which is understandable but more importantly aren’t “hungry”. They are too comfortable in a welfare program to summon the drive to break out of their situations. Assuming most of these guys aren’t addicted to Fentanyl, how much more difficult would finding work and housing be if they were.
Economy
“La vida es recia porque cuando eres pobre te humillan”
(the fast life because they humiliate you when your poor)
(thefenpubliccrisis .608 2) The Fentanyl Public Health Crisis, FBA NDCA ,12/29/2023
“but providing a basic income does not solve the problem of meaning. As well as needing the basics for survival, patients trying to put their lives back together need to find ways to reconnect with the world beyond their addictions.”143
“economic decline alone is not sufficient to cause an opioid epidemic… countries like Greece and Portugal, have suffered huge economic shocks in recent decades without a resulting opioid epidemic. A key difference between these countries and North America is that opioids have been used less in Europe. European doctors did not face the onslaught of Oxycontin marketing, opioid prescribing has been more tightly controlled, and the culture has not demanded the elimination of all pain and has not treated pain as the fifth vital sign.” AF 78
Insurance
“the authors asserted that “the overdose crisis is an epidemic of poor access to care.” As we have seen, methadone and buprenophine work. But almost four out of five Americans with opioid use disorder don’t get these treatments. And it is often “fragmented and difficult to navigate”. These issues are particularly bad in the US because of the way health care is funded, the marginalization of addiction care, and the severity of the opioid epidemic. Long wait lists are the norm for opioid substitution therapy across North America.” AF 98, 99
“unfortunately the availability of methadone and Suboxone programs in Alberta and many places in Canada is extremely poor. [but] detox beds are quite expensive, and we cannot begin to touch the demand for treatment that exists in the population. On the other hand maintenance medication therapy is remarkably cheap.” AF 99
“Even when patients get on to buprenorphine in the US, they often struggle to stay in treatment because of insurance and cost barriers.” AF 99
Drug companies defend“free enterprise” when it suits them
“She [Dr. Angell] saw drug companies put twice as much money into marketing as into research and drug development, focus on small tweaks to existing medicines, and fight price regulation on the on the one hand while encouraging stronger government protection of their patent rights on the other” AF 107
Healthcare/ Social Good
“is health care a commodity that should be delivered according to the ability to pay… or is it a social good that everyone should have, that should be distributed not according to the ability to pay but according to medical need? I [Dr Angell] came down in the second school very very firmly and more firmly as I went along, and I favor a non-profit single-payer system, essentially medicare for all in a non-profit delivery system… The vagaries of the U.S. health care system, and comparisons with those of every other industrialized nation, show that the profit motive is not a good basis on which to design a health care system. Similarly, the free market is not the right system to distribute addictive substances.” AF 110,111
“They identified two key factors in the US that are absent in Europe and that have contributed to this culture: direct-to-consumer advertising and private health care systems that incentivize quick ways to increase patient satisfaction.” AF 70
“even cheaper than heroin in the 1990s were prescription drugs paid for by insurance plans, which is why three-quarters of opioid users started with prescription opioids.” AF 74
[Don’t let the data deceive you, the data states that these prescription opioids were not necessarily prescribed to them.]
The association between prescribing opioid and addiction or adverse outcomes is also not the one-way, reliable link these “downward spiral” stories suggest. True, almost 80 percent of heroin users reported using prescription opioids first (according to US government statistics). And yet, in 75 percent of cases, those heroin users who did begin with prescription opioids (as well as, typically, other substances like cigarettes, alcohol, and marijuana) weren’t actually prescribed the drugs themselves. It is extremely rare that a pain patient without pre-exisisting risk factors for addiction or past use of other illicit or habit-forming drugs develops an opioid use disorder, leading them to problematic use of their own prescription or to shift to the illicit opioid market. In the small minority who do have those factors (of the already small minority of long-term pain patients like me unable to tolerate other treatments or for whom non-opioid treatments prove inadequate), the risk of problematic use is modifiable risk, manageable by education and good communication between doctor and patient. Even where such problematic use develops, it is by no means inevitable or permanent. OO93
“People who have abused prescription opioids are forty times more likely to develop a heron addiction than people who haven’t.” AF 75
Doctors say Medicaid coverage falls short of escalating fentanyl use, KOAA 5, 1/22/2024
(this is a very weird .656) This Is a Very Weird Moment in the History of Drug Laws, New York Times Podcasts, 5/10/2024
Portugal
(this is a veryweird .930)
(jellyroll .998) WATCH LIVE: Senate Hearing on stopping flow of fentanyl, The Hill, 1/11/2024
“Portugal's brand of decimalization is actually quite tame. Distributing and selling drugs are still crimes, and the police and courts go after dealers. There are no outlets selling legal drugs; there is no legal marijuana.” AF 131
Contrary to her side’s idolization of Portugal’s “paternalistic” model, it does not go far enough for Carlyn. “These participants are more critical of the Portugal model. They tell me and other journalists there that, partly due to its success in reducing injection drug use rates, this model has stigmatized injecting, driving drug users who persists in this practice into the shadows. They tell me that the rights-violating control exerted by law enforcement in other countries is replaced here in part by an overly medical model where substance use is pathologized, where all use is seen as addiction and mental disorder.” OO 294
*
In my paper Commercial Weed is Dollar General selling E Cigarettes I explain that drugs make us docile, suggestible, and lower our inhibitions. I learned this from Catholic scholar Dr. E Michael Jones and his work against pornography which is also an addiction. Dr. Jones suggests that pornography is used as a political tool to oppress citizens under the pretension of liberty. Dr. E Michael Jones writes on cultural-political issues with an emphasis on culture. Many among my generation who research these issues have come to this same conclusion: that promotion of recreational drug use is a political and cultural weapon.
(Keep Them Happy With Drugs And Computer Games | Yuval Noah Harari, Political Incorrectness, 3/23/2022)
Further reading: Drugs as Weapons Against Us, John L. Potash
I don’t believe our current government is serving us and I don’t believe it can be reformed. When activists march for “solutions” they condemn systemic injustice but their solutions involve more State intervention; To be free to distribute drugs and needles, but where do these safe drugs come from? Multinational monopolies paid by taxpayers to produce legal opioids and meth to distribute to “victims” of addiction. A great many of whom steal daily for drug money, party, burn bridges, betray their friends and family, neglect their duties, and live off others generosity until they are outcast, all so they could continuously pleasure themselves with drugs.
“they might have a heroin habit or a crack habit costing them several hundred dollars per day”. AF 127
Slow down making excuses for them, we have a long journey ahead! “Addiction” or “negative reinforcement” emerges after the fact. The consensus is that initial drug use is voluntary. Delineation is necessary as obscuring the initial cause (pleasure seeking) from the effect (dependence) is a common tactic. Logical fallacies litter these experts proofs such as how quickly this student dismisses the Temperance model (exposure theory). “This model suggests that mere exposure to drugs leads to addiction… the Temperance model of addiction is not effective in reducing the amount of drug use and abuse and should be replaced by any of the alternative models of addiction.” Models of Addiction Kirby Harris 2015
Notice how this model was easily dismissed and not for valid criticisms of the cause of addiction but instead all the effort (4/5 of the text) went to condemning the effectiveness of programs based on the Temperance model. This subpar logic is not criticized because it is what the establishment wants to hear.
Availability/ Exposure
“Courtwright concluded that availability is a key factor, echoing the observation of William S Burroughs, who wrote, “addiction is an illness of exposure. By and large those who have access to junk become addicts.” Courtwright wrote, “Over and over again the epidemiological data affirm a simple truth: those groups who, for whatever reasons, have had the greatest exposure to opiates have the highest rates of opiate addiction.” AF 72, 73
“The laws in Ontario had just changed so that alcohol was available in grocery stores. Previously, it was available only at government licqour stores known as the LCBO, run by the Liquor Control Board of Ontario...“I bought some booze, then I got on the cocaine, then the fentanyl. I spend like 600 bucks in three days. Now I’m broke. They wanted to kick me out of my housing, but they said they’d give me another chance.“...The effect of the increased availability of alcohol in Ontario is, I believe, a perfect example of the effect of availability of drug-use patterns. People with alcohol problems began to tell me that while they had learned to avoid the LCBO, they were now coming across big new wine and beer sections while buying their groceries; they were even being offered free samples on their way of the store. And the more they were seeing alcohol, the more they were using it.” AF 72,73
“In the community, violence, poverty, easy access to alcohol and drugs, and norms that favor substance use are most significant. That’s why laws that limit the opening hours and density of stores selling alcohol or other legal drugs can be very effective.” AF 170
“One lesson from the Iceland program.. “highlighted was the recognition that alcohol is a gateway drug.” AF171
A BDM shill admitting that exposure is a major contributing factor:
“the other 50% of the risk for addiction is due to a host of environmental factors, occurring through out a lifetime, that interact with an individual's genetic composition to render him or her vulnerable to addiction to a greater or lesser extent. Several types of environmental factors have been implicated in addiction, including psycho-social stresses, but by far the most powerful factor is exposure to a drug of abuse itself. Certain “gateway” drugs, in particular, nicotine, have been shown to increase one's vulnerability to an addiction to another drug. Moreover, there is increasing evidence that, despite a range of genetic risks for addiction across the population, exposure to sufficiently high doses of a drug for long periods of time can transform someone who has relatively lower genetic loading into an addict. Cellular basis of memory for addiction,” Eric J. Nestler
Psyop/ Ads
For Previous generations alcohol was the most common drug of abuse, again simply because of availability . My generation is steeped in many versions of pharmaceuticals, including amphetamines and the psychedelics which defined my parents generation. The history of dirty (cut) drugs is beyond my research. The governments involvement in dosing citizens without consent with LSD in those early years is well documented. Does the government create addicts? It certainly creates criminals by creating unreasonable laws. Does the private sector have an interest in creating addicts? The answer is easily found in “ask your doctor”-pharmaceutical commercials and celebrity endorsements for sports betting.
Child
(Silicon Valley)
We find CDC studies claiming drug use is down among school children over the past years, whether that's valid should only be viewed considering the uptick in depression, increased prescribing, and lack of detection and enforcement since the world changed in 2019 but that's not really interesting. How is the government compiling data? Perhaps because cigarette smoking is down they average that across all drug use or they started ignoring weed, I don’t know. What is certain though is among existing drug use there are more overdose deaths because the drugs are contaminated with fentanyl.
An article in Healio online, January 12, 2024 by Weldon and Friedman states that:
“Overdose deaths among high school-aged adolescents in the United States more than doubled between 2019 and 2020, researchers reported this week in The New England Journal of Medicine.”
“in an interview, Dr Joseph Friedman, PhD, MPH of the David Geffen School of Medicine at UCLA explains that “Counterfeit pills containing illicit fentanyl are driving much of this risk. Teenagers are more likely to use pills versus the powder forms of drugs — previously the main source of fentanyl. In 2022 5% of 12th graders reported nonmedical use of prescription drugs. Many adolescents may be unaware of the proliferation of counterfeit pills, believing pills they encounter to be safe”
Combine this fact with the shocking numbers 7 of 10 street drugs are contaminated with Fentanyl. It is difficult to decode some of these stats, other similar data states that a large majority of street drugs contain a lethal dose of fentanyl. For our purposes the exact figures aren’t relevant.
Up to one in FOUR middle and high school students are abusing Adderall, shocking NIH-funded study finds, CAITLIN TILLEY, 18 April 2023
A report last month found one in 10 teenage boys in the US were prescribed the drug — with those figures not counting many that are abusing it without a doctor's approval...In some US schools up to 25 percent of students are abusing ADHD drugs...The research found a contagion effect with students in schools where ADHD more likely to abuse the drugs by 36 percent — no matter whether they had a prescription themselves… [typo not mine] Prescriptions for Adderall soared over the last three years, and the surging demand combined with supply issues for manufacturers led to a shortage.
Further research: Sharp Uptick in Adderall Prescribing for Adults Ages 22-24 Amid COVID-19 Pandemic (this article actually claims for children and young adults patient volumes declined during the pandemic but these minor discrepancies are besides the larger point I am making,)
Significant Increase in Deliberate Self-Poisonings Among Adolescents During the Second Year of the COVID-19 Pandemic, J Adolesc Health. 2023 Aug;73
I recently watched a Netflix movie Take Your Pills, and was reminded of the mass rate of Adderall addicts among college students.
The BDM is quick to allege a genetic role! But societal factors, “the pandemic”, caused a surge in ADHD prescriptions? The fentanyl pandemic is far from over. Meanwhile advocates of the Brain Disease Model, in real time, stand aside and allow children's undeveloped minds to become hijacked by Adderall. What will become of these children when easy access to Adderall come to an end, when over-prescribing is restricted. The collateral damage will be terrible as tightening will force addicts to seek their party/concentration drug on the street. This is the basis of my claim that we have yet to witness the full severity of this epidemic.
Foster Kids Prescribed Psychotropic Drugs,ABC News, 12/2/2011
Check out the rest of the reporting; Overmedication in Foster Care l Hidden America: Generation Meds - PART 1/3, ABC News, 7/31/2012
Additional Resources:
https://www.ablechild.org/about-us/
https://www.benzoinfo.com/
Confessions of an Rx Drug Pusher, by Gwen Olsen
Mailer
Here in Sawyer, Michigan, January 2024, I grab the US mail and discover a glossy ad for recreational marijuana. This is the first such ad in the mailbox I have seen besides billboards increasingly littering the scenescape for months.
Industry is allowed to blatantly ignore the law when it coincides with the agenda, Marijuana is a scheduled drug. Yet in my U.S. Mail I find this promotion to buy federally illegal drugs. In Indiana where pot is still illegal, billboards advertise weed dispensaries here in Michigan. Months ago I attempted to raise awareness for my city, township, and county to curb the advertising of this industry yet this mailer has proven their indifference and cowardice to protect the public, no matter how easy and acceptable limits on advertising would be, local officials instead prove to have no backbone or independent thought whatsoever. They are merely ceremonial ribbon cutters for license plate readers and to grant “legitimacy” for unlawful armed enforcement of administrative policy.
Our governments adherence to individual rights and limitations on government will not soon be restored, I am not a delusional Trump-tard but the fact that we at one time had a platform to defend freedom is a verifiable fact. “The common law is the real law, the Supreme Law of the land, the code, rules, and regulations, policy and statutes are “not the law”, Self vs. Rhay Wn (2d) 261. “All codes, rules, and regulations are for government authorities only, not human/creators in accordance with God’s laws. All codes, rules, and regulations are unconstitutional and lacking due process…” Rodriques v. Ray Donavan (U.S. Deptartment of Labor) 769 F. 2d 1344, 1348 (1985).
What might follow the cartoon flavored marijuana mailers? What else is an illegal drug? Fentanyl.
Besides more mailers with greater psychological hooks shouldn’t we expect “harm-reduction” advocates to peddle their wares via the same pipelines?
Meanwhile the regime overlooks crimes of “harm-reduction” advocates promoting their services.
(312of3 .203) c 03 01 23 fentanyl cirsis 3, Veyeral Disease 1,12/30/2023
The Doctrine of the Lesser Magistrate (popularized by Matt Trewhella) is an acceptable strategy when it is implemented for the agenda:
“The tension in the United States is encapsulated in an October, 2018 exchange, when former Pennsylvania governor Ed Rendell announced that he had incorporated a nonprofit seeking private funding to open a supervised injection facility in Philadelphia, which at that time had the highest opioid death rate of any major U.S. city. This despite threats from US deputy attorney general Rod Rosenstein that if one opened it would be immediately shut down by federal authorities. “I’ve got a message for Mr. Rosenstein,” Rendell said. “They can come and arrest me first.” FI 272
Again I admit harm-reduction has some validity but did it work for Philadelphia since 2018?
“Two years after its launch, the Safer Opioid Supply policy in British Columbia was associated with higher rates of safer supply opioid prescribing but also with a significant increase in opioid-related poisoning hospitalizations.”
Nguyen HV, Mital S, Bugden S, McGinty EE. British Columbia’s Safer Opioid Supply Policy and Opioid Outcomes. JAMA
*
The letter from the former DEA heads and White House drug czars goes on to say that moving marijuana to Schedule III “would supersize the cannabis industry in the United States by allowing them to evade IRS Section 280E and deduct business expenses.”
“Not only would this mean that marijuana corporations would be able to deduct expenses for advertisements appealing to youth and the sale of kid-friendly marijuana gummies, but it would also dramatically increase the industry’s commercialization ability,” they said.
We understand that moving marijuana to Schedule III would not legalize the drug, nor allow its prescription,” the former officials wrote. “However, the change would greatly serve to benefit marijuana companies who would bypass IRS Section 280E and deduct business expenses, drastically increasing their profit margins. This means more advertising, commercialization, and normalization.”
IRS Code 280E prevents businesses from taking most federal tax deductions if they are marketing a Schedule I or II controlled substance; the existing industry thus incurs a significantly higher effective tax rate than businesses that operate in other sectors.
Marijuana Rescheduling Would ‘Supersize’ The Industry, Former DEA Heads And White House Drug Czars Warn Biden Administration,October 13, 2023, By Kyle Jaeger
*
What does this look like under monopoly capitalism? I propose it won’t be long until it looks like cartoons promoting “clean”needles, and “safe supply” fentanyl and meth splattered all over billboards and inside mailboxes and within schools? I believe it is probable “the left” will provide school children with needles next to condoms in schools, to say the least.
*
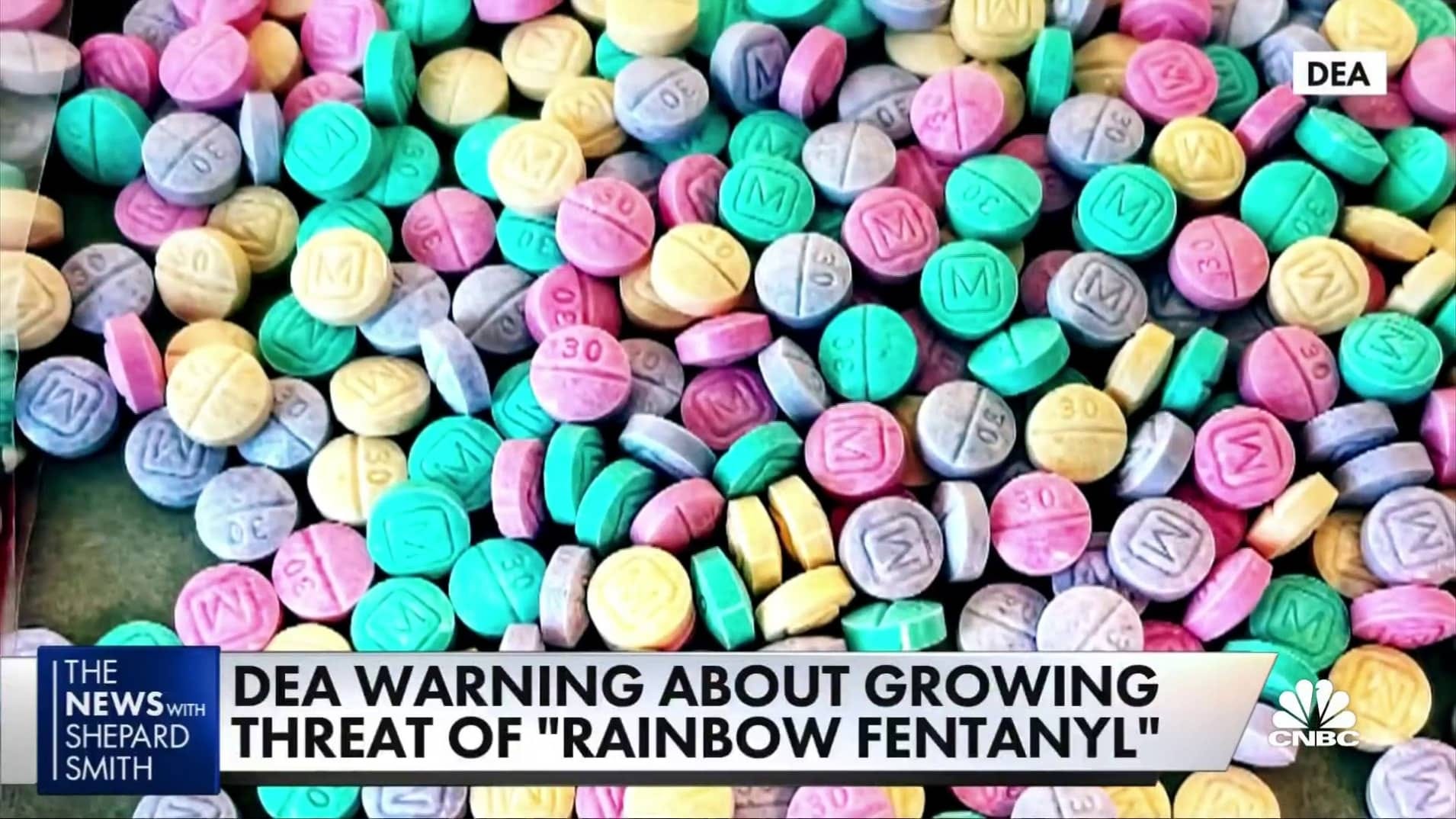
Whose idea is it to mass plaster photos of “skittles” everywhere as an ad campaign. Did nobody consider this could do more harm than good for the pre-literate and increasing number of children who don’t read (and infantile adults). Advertisers and psychologists know the power of logos, branding, and symbolism. I am not certain this campaign is malicious but on its face it seems possible that it is. Tell me you don’t want to eat these “skittles”.
*
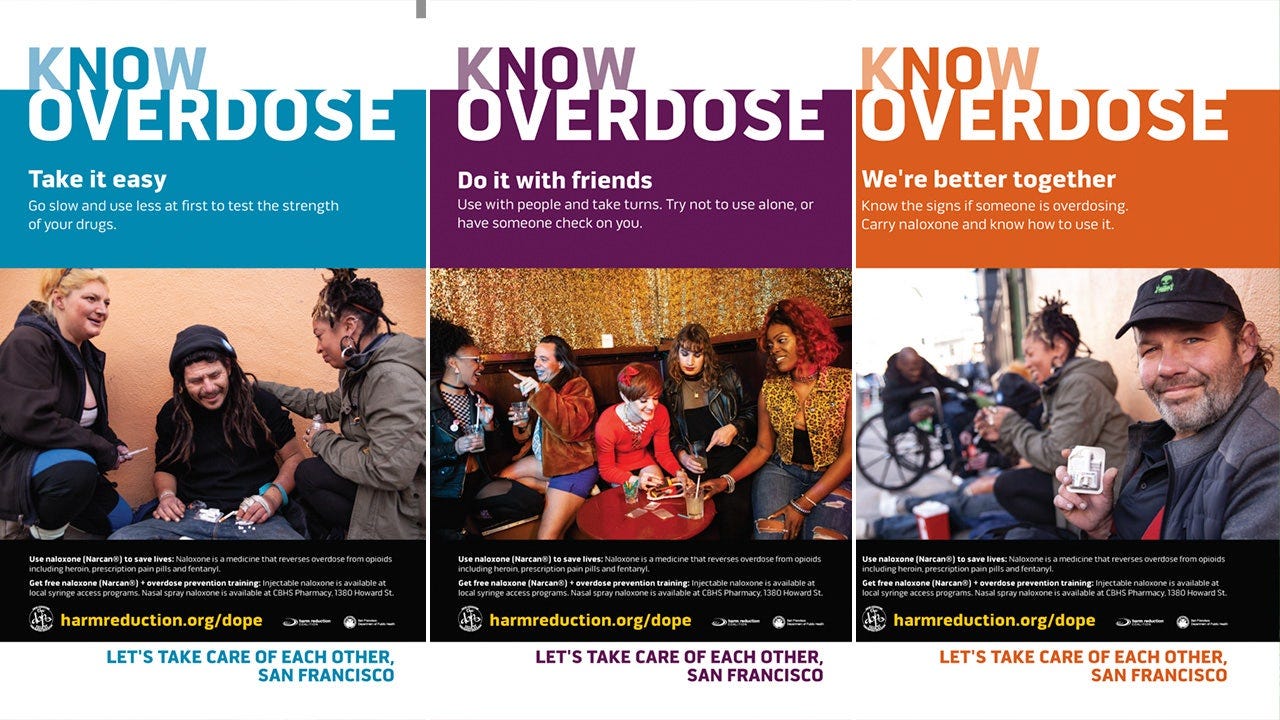
The general message carried by the San Francisco billboard appeared as well in the New York City health department’s “Let’s Talk Fentanyl” campaign, which last year told subway riders, “Don’t be ashamed you are using, be empowered that you are using safely,” and further counseled them to “start with a small dose and go slowly.”
The nationally influential Drug Policy Alliance goes further: It lauds many fentanyl dealers as “harm-reductionists” who should be respected and left alone by authorities (because the arrest of a trusted dealer might cause users to seek the drug from an unfamiliar source). A prominent subset of academics provides intellectual support for these initiatives, theorizing that stigma against drug use is ethically wrong and also worsens public health.
But destigmatizing the use of the drugs that are destroying their life is a profoundly mistaken approach.
Cultural disapproval of harmful behavior can be a potent force for protecting public health and safety—as the examples of increased stigma against drunk driving and tobacco smoking show.
Some harm-reduction services, notably needle exchanges and ready access to the overdose-rescue medication naloxone, do greatly help those who continue to use drugs. But most other arrows in the harm-reduction quiver are much less powerful, and as a primary response to the drug crisis, harm-reduction is plainly inadequate: Addiction and death rates remain appallingly high in areas that have shied away from tackling drug use and simply focused on reducing its harm.
And by definition, even a world-leading treatment-and-harm-reduction system helps only people who already use drugs. Because epidemics of any sort end only when the number of new cases declines, curtailing the synthetic-drug crisis depends on deterring people from using them in the first place. Destigmatizing drug use does the opposite.
Maintaining some modest penalties, particularly for public drug use, can help prevent use from being normalized. Mandated treatment for offenders with addiction problems would underscore societal disapproval while also helping those people—and their families.
Destigmatizing Drug Use Has Been a Profound Mistake By Keith Humphreys and Jonathan Caulkins
[I only agree with Keith Humphreys on some solutions]
*
The media worsened the damage of the tide pod challenge but doesn’t the state and media chose to not report stories if it may harm the public? Was The War Of The Worlds broadcast a psyop or an accident?
Film Theory: The Tide Pod Challenge - EXPOSED!, The Film Theorists, 2/13/2018
(Christoff .232) JASON CHRISTOFF ~“Mind Control Deprogramming From Global Lies & Egyptian Occultism”[Age Of Truth TV], Age Of Truth TV, 4/29/2024
State Targets Citizens
It is a centuries old myth that our form of government exists for the benefit of the people to protect our rights and property. The anti-federalists fought against the federal constitution which centralized power to Oligarchs. If you think our government today is in some way in opposition to the global regime which promotes woke ideology, sexual debauchery, and drug use then you are naive. Even if some politicians or bureaucrats do care they are not the majority in power and neither does it mean they know viable solutions but more likely as social-democrats they are swept into the popular “harm-reduction” ideology and conversely conservatives are led to press for stronger punitive actions no matter where the ax falls.

Conservatives who believe Fentanyl addictions and deaths can be slowed or stopped by this government are ignorant. Our corrupt bloated government cannot perceive, let alone implement viable solutions. Still today many imagine that the state cares about citizens. Disclosing my bias as a dissident from the onset is necessary. I claim systemic government corruption as a fact not an opinion.
*
(Canadian youth can now get ‘safer supply’ doses of fentanyl from the gov’, Jan 18, 2024, Straight Arrow News)
(Tucker Carlson - British Columbia pushing Free Fentanyl addictions!, Marcel Irnie, 1/26/2024)
(Is giving fentanyl to minors a good idea? Albertans react to BC's "safe supply" policies, Rebel News, 2/8/2024)
There are very few independent voices dissenting from the far-left harm-reduction narrative. I presume one reason is the sheer difficulty of untangling and explaining the intricacies as well as the need for restraint and nuance while placing value judgments on suffering addicts. With this paper i will fully engage the battle against both sides. Conservative thought leaders only highlight the absurdities because of the difficulty in defending a conservative position while the science is seemingly stacked against them. Their inability to address the science head-on is intellectual laziness which amounts to granted concessions.
Does science back the “moralist” stance against harm-reduction? Arguably No! But my perspective is based on first principles.
“Safe supply and other initiatives that make opioid use less dangerous intervene to prevent the fatal moment when the breath slows to nothing. These, and not the dreadful advice worried parents often receive to push their drug-using children out of the house, to cut off relationships, to stage humiliating and manipulate “interventions”, to discourage use of life-saving addiction medication, are what would have kept their deceased loved ones alive.” OO 103
“all evidence so far shows these facilities have proved incredibly effective at slashing over-dose deaths in every country that has welcomed them.” “Let cities open safe injection sites” New York Times editorial board 2-24-18
“Individuals who are engaged in agonist-based MAT (buprenorphine and methadone) report significant reduction in the aforementioned symptoms, feeling “normal” or “clear-headed,” and having an increased ability to focus on other areas of their lives… treatment to achieve better health outcomes.”
In 2017 American life expectancy declined for the third consecutive year, something that hadn’t happened since the 1940s. The CDC attributed the drop in part to fentanyl..Initially, New England states were most severely hit by the fentanyl crisis, but in 2017 Massachusetts, Rhode Island, and Vermont saw their overdose death rates decline, likely thanks in part to increases in addiction treatment programs and the public-health campaigns. “It could be an indication that increased access to treatment, safer use practices, and prevention methods are working,” said Mario Merno, former press secretary for the White House Office of National Drug Control Policy. A hallmark of Rhode Island’s strategy is providing access to opioids replacements for incarcerated people with additions, which appears to stop them from overdoing upon their release.. Ohio, a state whose Medicaid expansion in 2015 has given many users access to addiction and treatment programs, has also seen its overdose death rate drop dramatically in some of its hardest-hit areas. On the national level, the SUPPORT for Patients and Communities ACT, signed by Trump on October 24, 2018, was a step in the right direction in its provisions for better opioid treatment options, though greater resources are needed.” FI 273
HIV
One of the key health and economic benefits of needle exchange programs is in preventing the spread of HIV,” AF120
The HIV/ virus narrative is closely tied to harm-reduction. Instead of spending any time on it myself I will refer you to Dr. Sam Bailey in print Virus Mania or her videos on Odysee. Dr. Andrew Kaufman and Tom Cowan are the leading voices exposing the false virus narrative.
“Throughout much of the United States, it’s illegal to give someone a sterile syringe to prevent the spread of HIV or viral hepatitis; where syringe exchanges are allowed, it’s a strict one-for-one swap that sharply limits the disease-preventing value of clean needles, even though needle and syringe programs have been found not to increase drug use among participants, have been shown to promote lower-risk injection behaviors and, along with other harm-reduction measures, may reduce overall prevalence of injection drug use.” OO 99
(Germs Don't Cause Disease: Contagion & Virology Myths w/ Dr. Andrew Kaufman | 522, Luke Storey, 2/13/2024 x3)
Before the internet made research easy, in 1999 Stephen Fried wrote Bitter Pills exposing the dangers of Big Pharma because his wife was injured by the antibiotic Floxin. His finding are just as relevant today. My inclusion of his quotes are a great opportunity to encourage your own independent research because his is one book, one story in a sea of information. It’s hard to know when to end a presentation because the research can go on forever; this is why we should all maintain our own perspectives. Our own experience and resources are always different from others. Many researchers no matter how well read may never have come across Fried’s opinion. I feel unprepared I haven’t read Dopesick or The Least Of Us but I also can’t be expected to consume every single breadcrumb before forming an opinion! A lesson I learned a long time ago is if you wait for that day when you are fully prepared to launch your goal… that day will never come. Everything is an incomplete work. I have to stop myself from consuming more videos on fentanyl as time progresses to finish what I have already compiled. Researching and preparing this presentation has taken over eight months of my free time.
The dangers of Floxin did not disappear just because they were thoroughly exposed by Fried in ‘99.

“while pharmaceutical science has made some medical miracles almost routine, the sheer size of the legal- drug world means that its problem areas are bigger than the entire illegal-drug problem...
“For example, far more people die each year from adverse reactions to prescription and over-the-counter medications than succumb to all illegal drug use.. The estimates for U.S. deaths from legal drugs [written in 1999] represents 2 to 9 percent who die annually, thereby qualifying as at least the sixth leading cause of death in America, and possible as high as the third- behind only heart disease and cancer. ..but according to to studies in the JAMA, as many as 11 percent of all hospital admissions are the result of adverse drug reactions,.. More than one-quarter of all inpatients have adverse reactions to the drugs they are given in the hospital- many the result of presentable medication errors-which make ADRs the leading cause of in-hospital injury.” BP 5,6
[Flockhart] “knew that antibiotics, even though they are the second most commonly used class of drugs in the world, are improperly prescribed 40 to 50 percent of the time.. Apparently everyone in medicine knows this except patients.” BP 29
“Graedon hit the ground running with his pronouncement that more people died every year from adverse reactions to arthritis medicine than died from all illegal drug use (based on figures from FDA and a leading rheumatologist).” BP 117
Consider this as we discover that Advil and Tylenol are replacing opioids for genuine pain needs. I am personally convinced that opioids are less dangerous than liver killing NSAIDS.
“Kessler said that 90 percent of all adverse events involving drugs and devices, and perhaps as high as 99 percent of the most serious adverse events, were never reported to the FDA. The reason, he speculated, was then when doctors were confronted with an unexpected outcome of treatment, they were more likely to blame the event on “the course of the disease” than on the drug they had prescribed... “He was admitting that the FDA didn’t know nearly enough about the thousands of drugs the agency had already approved” BP 64 65
I would like to go into Kessler and Clinton and their relationship to Big Pharma but that is another story. I am told Drugs as Weapons Against Us addresses this. Among other points, Kessler vehemently suppressed Brezinski who had largely cured cancer.
“Anxiety drug pregabalin [Lyrica] killed my son — and hundreds more are dying from it”…“Originally a treatment for epilepsy, pregabalin now has the fastest-rising death toll of any drug in the UK. How did we sleepwalk into a US-style opioid crisis?”, Venetia Menzies, 03- 03-2024
State Targets Civilians

Police accused of 'mentally torturing' man in 17-hour interrogation, Published on 6- 4-2024 , FOX 11 Los Angeles
(gambling)
This attack against citizens voluntarily contracting via gambling is not based on morality. Sports betting and casinos are monopolies protected by the State. These attacks against this community are less to protect the monopolies but are an overt display of force to reinforce the states monopoly on violence. This is what law amounts to in this country, not morality nor necessity, but domination for no other purpose than reinforcing dominance of the State. I include this clip for the context. This is the same Regime advocates and politicians expect oppressed citizens to trust to cure their addictions.
I do foresee fentanyl as a great excuse for tyranny because many draconian measures can be justified in its name. Although I have no choice but to address laws surrounding fentanyl I still do not endorse any actions by the state. You may spot contradictions in my writings but this isn’t about my linear logic. This is about laying out the facts along with my educated opinion and defining the parameters so that you can decide what to believe for yourself. (Just as I promoted positive kratom legislation in my previous paper.)
(Blockchain Brain Boxing - Why Do People Continue To Disregard EHR and Wellness Impact Data? Alison McDowell, 5/22/2024)
Whatever the State attempts is usually a complete failure if not solely intended to further centralize power. What does this say about those in power who remain complacent? Our corrupt State’s only tool is force (besides withholding benefits). A society built on force and fear fosters a currency of ruthlessness, cunning, and corruption which creates recidivist violent criminals and often by mixing victimless criminals with violent ones.
(312of1 .474) c 03 01 23 fentanyl cirsis 1, Veyeral Disease 1, 12/30/2023
(312of1 .269)
(312of2 .205) c 03 01 23 fentanyl cirsis 2p, Veyeral Disease 1, 12/30/2023
(312of3 .920) c 03 01 23 fentanyl cirsis 3, Veyeral Disease 1, 2/30/2023
(howtheusguil .878 seg 3 seg 2) How can the US solve the Fentanyl crisis? | Sam Quinones, Giuliano Giacaglia,12/21/2023
measure of success a year in .142) A year of drug decriminalization in B.C., The Globe and Mail ,2/8/2024
Quinones has some good ideas but he does not have my approval:
(how overdose.420 seg 2) How Overdose Became America’s Silent Killer - With Sam Quinones, The Lonely Podcast ,12/24/2023
Quiones is Anti-Gun (howtheus .526)
Decide what to believe for yourself, but I believe my access to defensive tools should be equal to anyone elses.
[criminalization and prohibition] leads gangs and organized crime to the lucrative drug trade, and users commit property crimes to acquire funds to pay for drugs at prices that are inflated by scarcity and risk...Approx. one in five inmates in US prisons is inside for one or more drug-related crimes.” AF 126
(catotrump .070) Cato Daily Podcast, March 20, 2018, Trump’s Disappointing Approach to Opioids
(catotrump .443)
Cato is very active arguing for the same platform as the far-left. Singer provides many proofs against criminalization and argues for legitimate pain patients . Here are some other shows:
Cato Daily Podcast • January 31, 2019, A Challenge to Conventional Narratives on Opioid Overdoses
Cato Daily Podcast • June 1, 2021, Follow the Science on Opioids
Cato Daily Podcast • April 1, 2019, The Opioid Crisis Is Driven by Prohibition
Cato Daily Podcast • October 8, 2019, How the Feds Impede Evidence‐Based Opioid Treatments
Cato Daily Podcast • October 8, 2019, How the Feds Impede Evidence‐Based Opioid Treatments
Cato Daily Podcast • January 19, 2022, State‐Level Reforms for Addressing Opioids
Even Bernie Sanders calls some of these policies out; Bernie Sanders: "Open borders? That's a Koch brothers proposal", Vox, 8 years ago
China, Mexico
I have multiple clippings from my local paper of Indiana Prison correction officers convicted of smuggling drugs into the prison. If our State cannot keep the drugs out of prison what right does it have blaming China and Mexico especially while it allows illegal immigration. Similarly shouldn’t every state in which weed is still illegal be calling for border security on the Michigan border (where recreational weed is available for sale to out-of-state citizens). Why aren’t there calls to bomb the distributors of the federally illegal drug in Michigan? Selective enforcement?
I pass by new marijuana dispensaries every day where I live. They have a 24/7 armed guard presence on the property. In this light it seems odd that neither banks, liquor stores, nor pharmacies have full time armed protection. What does this tell us about the caliber of these dealers, their adversaries, and their profits.
(this is a very weird .833)
If you removed (necessarily by force) the majority of fentanyl from the street today users would not simply quit because of the inconvenience but instead commit greater crimes for the drug. Major trafficker’s profits would increase beyond that of the small scale providers, such as those who obtain drugs online ( Ben Westoff’ s example in my previous paper). Trump, and the county in which I live, proved this phenomenon with lock-downs. Main street suffered while Wall Street absorbed the profits. When the state targets even mid-level suppliers, which is the conservatives justification for continuing the drug war, the majority of prosecutions will be poor local addicts not the leading cartels.
What is the difference between the local poor user who deals to subsist and a terrorist cartel member?
We are supposed to belief the federal government will not target civilians. Crocodile tears Jaeson Jones uses teenage fentanyl deaths as the excuse to expand Federal powers.
(jaeson .351) The Fentanyl Epidemic: Jaeson Jones & Dr. Michael Jensen on What Must Be Done to Stop It, Real Talk,Published on May 15, 2024
Like 9/11 the only excuse these federal apologists can claim is incompetence, because the real causes of these “failures” is corruption, conspiracy, and treason.
(Jaeson .667, .879)
(Jaeson .142)
I agree with him in one regard which is that this is going to get a lot worse.
I have no faith or respect for this man who views himself and his government as a moral authority and his certainty of expanding the surveillance-prison state, again in the name of terrorism, makes him and his agenda very suspect.
(jaeson .647,.998)
“One of the harms is the geographic overlap between people recovering from drug use and people trying to sell drugs. Often, these people are the same people, just at different stages of treatment, because the best way to pay for a drug habit is to sell drugs. In practice, it means there is a concentration of drugs around addiction clinics and pharmacies.” AF 80
Poor citizens are always the intended target:
In Providence, Rhode Island, for example an undercover detective faked opioid withdrawal symptoms. In apparently desperate straits, he asked a man in treatment for opioid addiction if he had an Suboxone, an addiction medication that contains buprenorphine- and then arrested the man after he was sold a single film of the drug, a five dollar crime whose only effect would have been to prevent overdose death. A total of twenty-three people were ultimately entrapped by this cop and charged with narcotics trafficking for doing exactly the same, for the same piddling amounts.” OO 100
There are no top dealers:
(howtheusgiul .322) How can the US solve the Fentanyl crisis? | Sam Quinones, Giuliano Giacaglia,12/21/2023
(jaeson.332)
Further prosecution will only benefit those already above the law and increase prison profits. Only the most naive state apologists will deny government collusion with cartels. Remember the local correction officers smuggling drugs; are you gullible enough to believe those with more authority possess greater morality than the general public? Of course there are some dealers outside of state protection as is the nature of the black market. The government is limited in its capabilities because the State does not have a monopoly on violence against cartels. Real gangsters employ not weapons of home defense but weapons of war, weapons intended to fight governments (Many US citizens are too cowardly to admit the second amendment is a preventative against state tyranny and not simply for self defense against neighbors). Provoking a war against these cartels may teach the world how ill equipped our state is to deal with real organized violence. The state is most accustomed to targeting innocent civilians. How long until cartels begin forcefully extracting their own from Americas prisons?
At least a dozen dead in northern Mexico shootout near Texas border, By Reuters, February 19, 2024”
Soldiers and civilians are dying as Mexican cartels embrace a terrifying new weapon: Land mines, By Keegan Hamilton and Kate Linthicum, Los Angeles Times
San Jose Police Union Executive Charged With Attempted Illegal Importation Of Fentanyl Analogue, Wednesday, March 29, 2023, U.S. Attorney's Office, Northern District of California
CATO defends open borders; Fentanyl Is Smuggled for U.S. Citizens By U.S. Citizens, Not Asylum Seekers,By David J. Bier
But the rest of the story is cartels pay US citizens.
Mexican cartels recruiting US soldiers and other Americans for their dirty work, Current and former military members among those that have acted as hitmen and smugglers on behalf of criminal groups, Sara Ruthven
An academic book on the corruption of government involved with cartels is Drug Cartels do not exist, Oswaldo Zavala
The Politics of Heroin, CIA Complicity in the Global Drug Trade, By Alfred W. McCoy
“In contrast, [Gary] Webb has made other statements all but stating that the Dark Alliance series did demonstrate CIA involvement in the spread of crack in America. In September 1996, in the immediate wake of the Dark Alliance series, [Gary] Webb reportedly posted the following comment on the Mercury News electronic bulletin board: "One thing I did want to respond to directly is the writer who claimed there wasn't any 'proof ' of CIA involvement in this thing. That's like saying there's no proof of General Motors involvement in making Chevrolets.'" THE CIA-CONTRA-CRACK COCAINE CONTROVERSY:,A REVIEW OF THE JUSTICE DEPARTMENT'S INVESTIGATIONS AND PROSECUTIONS, https://oig.justice.gov/sites/default/files/archive/special/9712/ch01p1.htm
American War Machine,Deep Politics, the CIA Global Drug Connection, and the Road to Afghanistan, Peter Dale Scott
(jaeson .445, .994)
High level dealers and gang leaders will be the least affected by tougher laws. Every aspect of their existence is criminal from weapons to human trafficking, to expect tougher penalties to dissuade genuine gangsters is merely an excuse for increased tyranny against helpless poor civilians.
(cartel carol) Carol does YouTube lives of aggregate news every night; neverlosetruth5
Treaty
“The [Congress are} vested with the great and uncontrollable powers,.. And are by this clause invested with the power of making all laws, proper and necessary, for carrying all these into execution; and they may so exercise this power as entirely too annihilate all the state governments, and reduce this country to one single government. And if they may do it, it is pretty certain they will.” ‘Brutus;” Essay 1, 18 October 1787
“The Senate, by making treaties may destroy your liberty and laws for [lack] of responsibility” Patrick Henry, Virginia ratifying convention, 7 June 1788
“Jefferson writes regarding the Federal government against the “Implied powers” doctrine, “To take a single step beyond the boundaries thus specially drawn around the powers of congress, is to take possession of a boundless field of power, no longer susceptible of any definition… In like manner they are not to do anything they please to provide for the general welfare, but only to lay taxes for that purpose.” Hologram of Liberty, Kenneth W. Royce, Pg 89
Moving Marijuana To Schedule III Would Not Violate International Treaties, Legal Opinion Says, February 13, 2024, By Ben Adlin;
“A group of lawyers argues in a newly released legal opinion that contrary to what the Drug Enforcement Administration (DEA) has asserted in the past, international drug treaties ought not stand in the way of moving marijuana to Schedule III of the Controlled Substances Act (CSA), as the Department of Health and Human Services (HHS) has recommended.”
An argument by a group of lawyers doesn’t change the law. The existence of this article at this time is proof that currently marijuana is a violation of UN treaty or they wouldn’t be arguing the fact.
The opinion is intended largely to refute a position DEA took in a 2016 denial of an earlier marijuana rescheduling petition, in which the agency wrote that “in view of United States obligations under international drug control treaties, marijuana cannot be placed in a schedule less restrictive than schedule II.”
“claiming that any reclassification that puts marijuana outside of Schedule I or Schedule II “would constitute a violation of the Single Convention,” referring to the 1961 United Nations (UN) Single Convention on Narcotic Drugs.”
In addition to the legal opinion’s arguments that the drug treaties don’t preclude moving marijuana to Schedule III and that the lower classification actually better fits the spirit of the international agreements, it also claims member countries aren’t bound by the treaties when doing so would violate their domestic constitutional frameworks.
The treaties, lawyers wrote, “include exceptions when a Party is bound by constitutional limitations, and shutting down the State adult-use Marijuana markets on Treaty grounds would intrude into core police powers reserved to the States under our Constitution.”
As Hauser sees it, current treaties already allow flexibility for countries to regulate drugs for certain purposes, like medicine and scientific research, instead of prohibit them outright. That should be sufficient to allow moving marijuana to Schedule III, as she believes the U.S. is already signaling on the international stage.
Especially as conversations turn from medical legalization to broader adult-use—and potentially to regulation of psychedelics—international drug treaties crafted during an era of near global prohibition might need to be revisited and revised.
Meanwhile, six former DEA heads and five former White House drug czars sent a letter last October to the attorney general and current DEA administrator voicing opposition to the top federal health agency’s recommendation to reschedule marijuana. They also made a questionable claim about the relationship between drug schedules and criminal penalties in a way that could exaggerate the potential impact of the incremental reform.
Two GOP senators, including the lead Republican sponsor of a marijuana banking bill that cleared a key committee in September, also filed legislation late last year to prevent federal agencies from rescheduling cannabis without tacit approval from Congress.
And a coalition of 14 Republican congressional lawmakers separately urged DEA to “reject” the top federal health agency’s recommendation to reschedule marijuana and instead keep it in the most restrictive category under the CSA.
A recent poll found that about one-third of marijuana consumers say they would go back to the illicit market if cannabis was rescheduled and only made legally available as a Food and Drug Administration- (FDA) approved prescription drug.
(David Knight 21)
Harm reduction

[Baluard, a center in Barcelona] also advertised are workshops on how to administer Narcan and how to convert cocaine to crack, so it can be smoked instead of shot up, which has some health benefits.” AF 268
Crack is safer than cocaine?
[harm-reduction] practices are often very controversial.. they are associated in many people’s minds with a dubious, left-wing political program that seeks to turn attention away from individual responsibility or morality and toward social, political, and economic factors… which assign some people greater power in society than others, dramatically determining health outcomes as well as how drug laws are created in the first place, and then how they are selectively enforced to preserve an inequitable status quo.” OO 107
“An example of harm-reduction that is well accepted by most people would be the laws we have requiring seat belts in cars.. they allow us to continue the intrinsically dangerous activity of driving by significantly reducing the harms that may result from a crash.” OO 106
Carlyn is clever but intellectually dishonest; driving cars is not illegal nor immoral. If the actions were legal then they would be regulated. Fentanyl use is not legal.
“bereaved family members are also angry at physicians who may have prescribed a drug they see as the start of addiction; the drug companies and marketing executives that maximized profits while minimizing public understanding of how opioids work and coaxing doctors to prescribe them; at the friends who may have bought or shared drugs or enabled their loved one’s drug use...But other grieving parents feel equally betrayed by the language of tough love, by the advice to avoid “enabling” and let one's loved one reach a completely mythical “rock bottom”...Shultz (a bereaved mom) learned [from Johann Hari’s Chasing the Scream] “that there has always been a tight connection between race relations and drug war policies, that human rights of drug users are routinely violated, that it’s not just that people who use drugs are burdened with dependence on a dangerous substance, but that the substance is dangerous in large part because they are alienated from families and communities by criminalization or terrible treatment regimens or poverty or shame...Rather than joining drug warriors like many other bereaved parents [they] decided to work in solidarity with drug user unions and harm-reduction advocates. [they] push for decriminalization as well as harm reduction initiatives including safe supply...Safe supply and other initiatives that make opioid use less dangerous intervene to prevent the fatal moment when the breath slows to nothing. These, and not the dreadful advice worried parents often receive to push their drug-using children out of the house, to cut off relationships, to stage humiliating and manipulative “interventions,” to discourage use of life-saving addiction medications, are what would have kept deceased loved ones alive...So-called tough love, Schultz says, alienates people who use drugs without either dealing with the reasons they use, or providing help with the withdrawal and cravings that so frequently lead people pushed into abstinence back to the drugs, and to fatal relapse, with no further chances. OO 102-103
The greatest profits are found in government contracts. What better pretense than to claim the yoke of charity and morality to argue for addicts who have no valid justification to remain addicts other than the discomfort of quitting. You don’t die from quitting, withdrawal from Fentanyl is not fatal. Relapsing may be dangerous but so is continued use.
(christoff .775)
(powdered fent def .368) Powdered Fentanyl - The New Safer Supply on the Block, British Columbia Centre on Substance Use, 4/23/2024
Weed stores are already a distribution center for harm-reduction supplies. Is “harm-reduction” not an industry in itself? What a perfect job for an unskilled but over-schooled social justice warrior:
-easily gained status and prestige among the most desperate
-discretionary power over controlled substances and paraphernalia
-educated in social sciences to spoon feed the latest methods of surveillance and medical intervention
-as a narc, an intermediary between users and the militarized police-prison industrial complex
There is no shortage of woke status-seekers with masters degrees looking for work, no shortage of grant writers fully submissive to the post-modern intersectional-victim welfare state. Societies investment in their college debt was to hand out clean needles while they self-righteously march for bio-metric fentanyl vending machines!
Harm Reduction is Not Prevention
”We want to feel some kind of rush”. The goal is to support patients in abandoning the contaminated, untrustworthy illicit opioid supply, rather than in setting abstinence-based goals that are then routinely broken because the patients are not able or willing to meet them. Methadone or buprenorphine, of course, are effective, life-saving, and well-evidenced treatments for many opioid use disorder patients. But other opioid users in treatment routinely supplement these prescribed medications with street opioids because although methadone and buprenorphine prevent withdrawal, they don’t provide the high… these treatments can be a pale substitute for what you really need.” OO 244
(ep2the .428) Ep. 2: The Fentanyl Treatment Keeping People High, Discovery Institute, 5/29/2024
These activists have been known to buy drugs from suspect sources, so “safe” is doublespeak. We have recently seen these same advocates (they cross promote each other) adopt the same solutions across borders such as BC providing Fentanyl to minors without parental consent. There is no accountability, no rule of law, local or international. Denying the rights of parents and legally accepting the consent of minors is evidence that our state has no legitimacy.
Read my older article https://mattcircus.substack.com/p/a-minor-discrepancy
Safe supply’s ultimate crescendo is Big Pharma billing tax payers to distribute drugs of abuse to drug abusers;
“imagine that you make a range of opioids available- ensuring lower-potency opioids like heroin are as affordable and accessible as illicit fentanyl. This would begin to open the possibility for people who are dependent on very high doses of illicit fentanyl to gradually lower their tolerance and move from the dangerous illicit supply on the street to lower-strength, regulated heroin...
“There’s groups of us who don’t want fentanyl, “Lauren tells me. We’ve got to stop the bleed [from illicit fentanyl overdose]. We go from fentanyl backwards.” OO 300
Gender affirming care
"evidence-informed approach" instead of an evidence-based approach”
Gender-Affirming Psychiatric Care," just released on Amazon at $58, is a textbook printed by American Psychiatric Association (APA) Publishing...the textbook signals early on that it's more subjective than objective, quoting a feminist studies professor saying, "Scientific neutrality is a fallacy."..The textbook's introduction says the book is based on an "evidence-informed approach" instead of an evidence-based approach, which is more scientific, ...said Dr. Lauren Schwartz, a psychiatrist in Oklahoma speaking out against the rush to "transition" children...she told The Epoch Times. -New Trans Textbook for Psychiatrists Could Harm Millions of Kids, Critics Say Authored by Darlene McCormick Sanchez via The Epoch Times
An argument whether science itself is value- neutral is beyond my capacity. But here is one clarification; “Claims about the value of science and technology once realized focus on the consequences of scientific and technological activity and the value of those consequences. In this context those who make claims about neutralism assert that scientific and technological activities merely create possibilities but do not cause any specific possibilities to be realized. To actualize any of those possibilities, other events beyond science and technology are needed,” https://www.encyclopedia.com/science/encyclopedias-almanacs-transcripts-and-maps/neutrality-science-and-technology
I follow up with an allegation that the authors of the Gender Affirming text book refuse to acknowledge their own biases influencing their work while they make abstract claims for all of “science”.
I will use the ideological-left’s own arguments against them. Dare I suggest most harm-reduction advocates subscribe to many of the same tenets, which is best exemplified in their cross- promotion of birth control.
“is based on an "evidence-informed approach" instead of an evidence-based approach”,
Evidence favors many harm-reduction solutions; harm-reduction saves lives and prevents spread of disease. These facts currently stand alone as grounds for implementing harm-reduction policies. But deconstructionists apply hyper-criticisms only to their opponents while they’re not equally critical of their own claims and assumptions. For the authors of this “social justice” text book it becomes standard policy to dismiss evidence that doesn’t fit their agenda or more specifically ignore solutions based on evidence if they don’t like the solutions; then they only consider the evidence instead of strictly following a compulsion to act upon it. I am proposing conservatives accept this argument. I oppose all but a few harm-reduction solutions. I reject most of their solutions on principle despite their evidence. My position is also “evidence-informed”.
I also came across another way advocates diminish the role of evidence or in this case proceed ahead without it:
Programs which are “evidence-generating” (powdered fent evidence.png)

To correctly convey this point I need a logistician or epistemologist. Just because something works doesn’t mean it is right. There may be hidden factors or external/secondary consequences missed. Solely because some isolated benefit is achieved through highly controlled experimentation doesn't necessitate their conclusions are above criticism. Whereas when things are universally True and Good they are most often accepted without debate (vegetables are good for you). Harm reduction solutions are highly contested.
(addictionspecialist .654) Addiction specialist blames “safe supply” for spike in fentanyl use, True North, 6/16/2024
(addictionspecialist .399) Addiction specialist blames “safe supply” for spike in fentanyl use, True North, 6/16/2024
notice Dr. Sharon Koivu rejects safe-supply but not MAT (buprenophrine) unlike Ginny Burton; a difference worth noting which you will have to decide for yourself.
Ginny is an absolutist against pharma-drugs to treat opiate use disorders. Not only is she against buprenorphine and all opioid therapies but she is also against Naltrexone because Industry profits from it. I also happen to be an idealist but I still have to function in society. As idealists we can hold ourselves to higher standards and we often voluntarily suffer for our values but that is our personal choice; we cannot expect others nor force others to adopt and implement our ideals. As far as Naloxone; it is virtually harmless as far as pharma-drugs go. My platform is not against Narcan or drug checking/test strips and even leaves room for responsible MAT, instead my platform targets the ideology behind these tools, that ideology determines how these tools are used.
“For him [Stefan Kertesz], evidence isn’t just throwing controlled studies around (x percent of people who take prescription opioids ultimately develop an opioid use disorder; more people who take the equivalent of 90mg of morphine daily run into problems than those who take less) to prove a point (taking prescription opioids for pain leads to addiction; daily doses of 90mg or higher are a bad idea for any patient). All the relevant evidence must be considered to grasp what’s going on, and numbers must be put in context (x percent of any group of people will go on to develop a substance use disorder; similar factors predispose people to addiction and to pain; over time, the effective dose of an opioid is expected to rise; for a small group of pain patients, opioids represent the best possible balance of benefits and harms). “ OO 132 133
FORCED JAIL
What if an argument was based on the fact that people who are jailed and without access to candy are healthier? In the name of public health, can’t this fact justify locking up overweight citizens, perhaps even citizens with a potential for abuse, maybe anyone who possesses certain genetic markers? Luckily other factors, such as our legal tradition which limits government, plays a greater role than any “evidence-based” solutions even if jail factually provides a diabetes free outcome. Scientism and technocracy might use a similar excuse to impose forced state interventions. Fentanyl provides easy excuses and defenseless targets (addicts). The homeless and prisoners are the least able to defend their rights. Even I can agree forced incarceration may be required to break fentanyl addiction.
In fact this argument is made by Volkow “Addiction doctors should be involved in the obesity epidemic; this is an addiction problem,” she proclaimed. [Dr. Brodie Ramin continues] Restricting access to harmful substances, by contrast, reduces consumption. So, exposure is the problem. AF 72
Researcher Allison McDowell researches surveillance technology. I include her in my writings as much as possible. She exposes the future of medicine, don’t fool yourself into thinking addiction medicine will be any different.
(Bobbygoes merged) Bobby Goes Ape Signaling Austin's Lunarpunks, Alison McDowell , 5/21/2024
Lulu 25 Days Sober & Off The Streets!!!!!, Lost in Phoenix, 2/18/2024
(how the us guil .438) How can the US solve the Fentanyl crisis? | Sam Quinones, Giuliano Giacaglia, 12/21/2023
(this is a very weird .131)
Naltrexone
(c06023 .203) c 06 09 23 opioid crisis 2, Veyeral Disease 1, 2/29/2023
“The naloxone passes right through the body if the tablet is used properly, but if someone tries to inject it, the naloxone is activated and puts them into immediate withdraw.” AF 92
“there is one that seems to be popular with authorities – the correctional system, for example. That’s naltrexone (sold under the brand name Vivitrol). Its hard to see it as coincidental that naltrexone has a distinctly punitive effect. To start it safely, you must first “detox”- that is undergo painful, unpleasant withdrawal for up to ten days- and then only start naltrexone when you no longer have opioids in your system. And then when you are using it, it blocks the effect of opioids like heroin. If, frustrated at not being able to get high or unable to cope without whatever opioids did for you, you stop taking naltrexone, you are then at far higher risk of overdose, and of fatal overdose, than before you detoxed. This is because while you had no opioids in your system, your opioid tolerance naturally dropped. And in fact, naltrexone has, for these reasons, been found to be ineffective at preventing overdose death.” OO 100
In my previous paper I lay out how Suboxone and to a lesser degree naltrexone (without wrap-around services and without “housing-first”) is the only scalable solution (I may have put too much emphasis on Naltrexone as a single solution). Abstinence is seldom considered anymore especially by harm-reductionists, instead they defend lifelong legal opioid prescriptions as “treatment”.
In this same video we find they can’t conceal their own contradiction
(Echo .345) HR ECHO | February 1 | Boogiemen and Zombies in the Era of Fentanyl: Six Myths about Harm Reduction, Be Well Texas, 4/15/2024
(echo .699)
Therefore Prevention deserves the leading role as the solution. Harm reduction promotions such as safe injection sites, destigmatization, safe-supply, and maybe even Narcan and drug checking (test strips) may provide a false sense of security and contribute more harm than good. I find myself in defense of test strips because experimenters who do not want fentanyl then have a means to detect and reject contaminated drugs. We shouldn’t conflate other drug use with fentanyl. A blanket condemnation of all drugs with a potential for abuse would rightly include cigarettes, weed, and alcohol. And may even include process addictions such as gambling and pornography.
(This is a very weird .419)
What are our leaders doing for prevention? The money is spent on Narcan, Narcan is not prevention for drug-use it is harm-reduction. It may prevent death but does not prevent initial drug use. More harm-reduction is more spending within the medical industrial complex. In my last paper TITLE I promoted giving our opioid settlement money freely to community organizations no matter how distantly related to this issue. I proposed the county pay for a trade school for me or my drug damaged peers who were given Xanax and Adderall by the schools. I stand by that as an only solution. I previously included the Iceland model.
“Intensive or less intensive behavioral health treatment, inpatient detox, or abstinence-forcing medication naltrexone (Vivitrol) – these popular, prevalent “treatments” are not treatment at all: they simply do not prevent overdose or death. In the case of naltrexone, you'll recall, it may in fact hasten it.” OO 115
“75 percent of the patients who had received buprenorphine were still in treatment, but all patients taking the placebo had dropped our of treatment, despite the groups and the counseling” AF 93
In a perfect world every user should have access to the best tools for recovery which includes Suboxone. But this ignores differences between tools, people, or situations. Yes, Suboxone is most effective at preventing relapse. However some people would prefer to not revert to legal opioids (buprenophrine) and instead chose a plan of abstinence although it is difficult but not impossible to attain. Buprenorphine is generally better than methadone, but still some prefer methadone. This issue is debatable, the stats go both ways. I just found stats that methadone is better, the value of either depends on your criteria; YouTube, Exploring the impact: a clinical study of fentanyl use in vulnerable populations, Addictions and Concurent Disorders Research Group 6-4-24.


Conversely;
“By some accounts, methadone is said to be even more difficult to kick than heroin and remains controversial in the medical field.” What Are the Worst Drugs To Get Addicted To?, Danielle Robinson, June 13, 2019
“guidelines now recommend buprenorphine as a preferred medication for opioid use disorder because the overdose risk is about six times less with buprenorphine than with methadone” AF 91
Conversely;
“82% who quit methadone relapsed after 12 months” AF 90 (this stat from 1988 is about heroin because not many studies are out about fentanyl even today, Reducing the Risk of AIDS Through Methadone Maintenance Treatment, John C. Ball, W. Robert Lange, C. Patrick Myers and Samuel R. Friedman, Journal of Health and Social Behavior)
Remember Fentanyl is in a league of its own, i would argue exponentially worse than heroin in every way. To lighten the mood I might say; if heroin is the extract of poppy then fentanyl is the extract of heroin. Although not scientifically accurate for our purposes it is.
“A young man with pink cheeks, a boyish face, and brown curls told a documentary crew in Calgary in 2016, “It doesn’t last long so you’re sick again; heroin you can do in the morning and you can be all good until tomorrow, [but with] fentanyl you can withdraw three times a day.” pg 62
Naltrexone is more effective than placebo, and it carries other benefits such as no potential for abuse and is a more accessible tool which can also be prescribed for alcoholism and overeating.
The naltrexone injection is the newest medication for the treatment of OUD. It was FDA-approved in 2010 and it is marketed to suggest that it can help reduce cravings- possibly due to the knowledge opioids will not work with the medication rather than an actual pharmaceutical effect; however, more research is needed...
Individuals using injectable naltrexone cannot have opioids in their system for at least 7-10 days as an individual would immediately go through withdrawal, so in most cases, medically managed detoxification is appropriate. If someone uses opioids while the naltrexone injection is active in the body (28 days after time of injection), they will not experience any effects from the opioids. However, after the 28 days, the medication is no longer active and the individual is at risk for overdose and death. The second component of MAT is behavioral therapy...
Behavioral therapy is required by federal law whenever medication is used to relieve withdrawal symptoms and cravings. Fewer than 90 days in treatment is not associated with positive outcomes…
oral naltrexone is generally not recommended as an appropriate treatment for OUD...
naltrexone is such a strong antagonist, so it may reduce tolerance even further than individuals who are abstinent without naltrexone...
There is lower retention in treatment with extended-release injectable naltrexone than with methadone or buprenorphine.[82] Education around the increased risk of overdose after a period of abstinence is highly important.”An Overview of Medication-Assisted Treatment for Opioid Use Disorders for Criminal Justice-Involved Individuals, Jessica Reichert, Lily Gleicher and Elizabeth Salisbury-Afshar|2017-07-18| ()
…“Behavioral therapy is required by federal law whenever medication is used to relieve withdrawal symptoms and cravings. Fewer than 90 days in treatment is not associated with positive outcomes”
I don’t know what to make of this. I can’t research every claim. Keep in mind that fentanyl is not subject to previous conclusions based on heroin and pain prescription opioids. I recognize the need for behavioral therapy but studies suggest that it is not necessary and in my opinion it’s not possible to address every one. What makes woke psychologist shills any more qualified than peers at an AA meeting, is it the six figure income they receive “toeing the line”? Wouldn’t they also advocate medically assisted suicide to forward the agenda?
Naloxone and Narcan have the same active ingredient but are used differently.
What happens after Narcan, after precipitated withdrawal? This is the best time to impose treatment. They are very sick now, Nacan caused severe withdrawal, so they seek fentanyl as soon as possible? Won’t they go to the nearest source, even their last supplier? Their tolerance is greatly decreased after Narcan exponentially increasing risk of overdose.
Controversially (as a classical liberal), I believe users should be institutionalized if Narcan is required. If life saving intervention is necessary aren’t addicts beyond their ability to care for themselves, aren’t they a danger to themselves? A lot is known about buprenorphine induction. I am not sure if you can completely prevent fentanyl from binding to the receptors with buprenorphine but i believe so.
(OUPC 2023: OAT in the time of fentanyl, CAMH Professionals Videos, 4/21/2024)
Can we give these addicted patients long acting buprenorphine and court-order them back for their next dose, if necessary tether them?
(treat and street clip)
Options like naltrexone and other detox issues, like seizures are also best addressed while institutionalized. I am not against compulsory extended-release naltrexone; I think it is a perfect policy for conservative hardliners who want to brute force the issue.
(This is a very weird .131)
(Live alaska .370)
(live alaska .298)
Dr. Ardis Nicotine
https://thedrardisshow.com/free-patient-resources
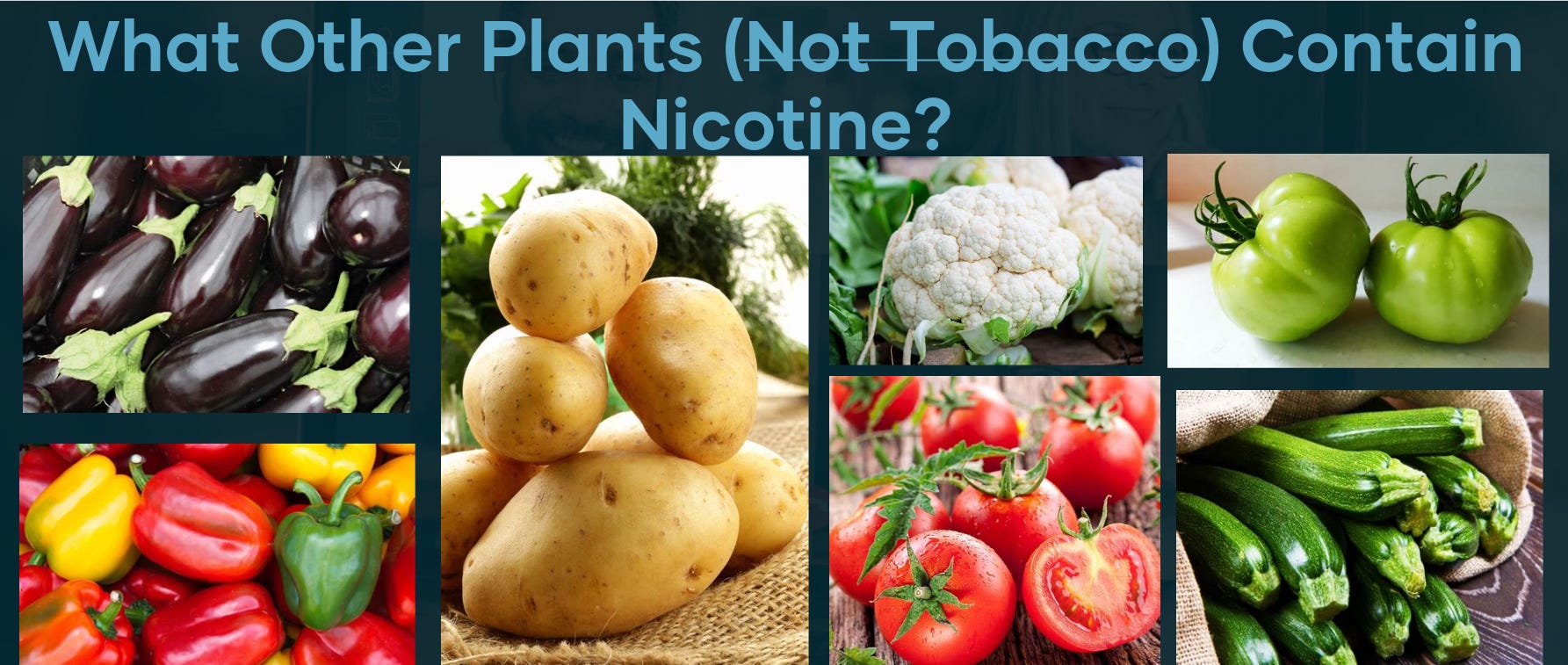

Nicole Discovers Ozempic
A YouTube creator named Nicole recovered from meth and opioid addiction. She continues to study these issues and has a job and certificates in the field (I oppose giving recovered addicts authority). She vehemently defends her current addiction to Suboxone. She is scared that if she quits she will relapse. She is also aware of the mental “dulling” effect that accompanies Suboxone as well as the physical repercussions which also effect the thyroid.
Other adverse effects include: “ We know for example, that long term use can cause reduced function of testes or ovaries, or low testosterone, which in turn may cause other problems such as low bone density… constipation” OO 312
I’m not a fan of her personality but of course I look to the fruits of her labor and she has valid insights and puts in the effort to study these issues. I don’t bring up discoveringnicole’s channel as an endorsement, she annoys me. Nicole is overweight and enjoys binge eating, a sin many are guilty of including myself. She recently began vlogging about Ozemic. Whether she endorses Ozemic or not for weight loss is irrelevant because she certainly sings its praise on account of her recent diagnoses of diabetes. Nicole is quick to defend against detractors who criticize her use of the new miracle drug because she is “diabetic”. Like BDM proponents, Nicole can claim victimhood and helplessness in the face of a disease. Obviously its irrelevant that type 2 diabetes has been studied for decades by alternative health advocates who have discovered that it almost entirely reversible by way of quality and quantity of carbs (vanadium and chromium, Dr. Jason Fung) but still today aren’t conscious of the difference between the glycemic index and glycemic load. There is a wonderful free video on YouTube Diabetes Free In 30 Days another great movie along the same lines is Chris Carr’s Crazy Sexy Cancer. This work is so overdone that my efforts lie in criticizing vegetable oils and fake vitamins because type 2 diabetes is solved as far as I’m concerned. I promote Dr. James Roberts information addressing Heart disease.
The Dangers of Industrial Fats & Oils, Liquid Polyunsaturated Oils & Solid Partially Hydrogenated Trans Fats
https://www.westonaprice.org/wp-content/uploads/IndustrialFatsOils.pdf
So Nicole rationalizes or justifies her use of Ozempic because she reached some arbitrary threshold of insulin disregualtion in which she qualifies for a medical label and according to her that label now relieves her of her duty of taking responsibility for her health and allows drugs to fill the need. Even if the drug had no negative side effects, which of course it will prove to, what she is avoiding with her drug use is not only the tedious research and digging (that she is willing to do for her illicit drug interests) which would then amount to promotion of quality ingredients such as low-carb recipes and promoting allulose but she also deprives herself of the spiritual growth that accompanies self control. Instead she belligerently defends her drug use just as she defends her addiction to Suboxone. Her ignorance or rather her stubbornness to admit any validity for an abstinence based lifestyle has led her to ignore a powerful tool she should be concerned with mastering and that is naltrexone, which is also used for overeating.
Does the sin of gluttony no longer require repentance, sacrifice, study (a great podcast is called Shortcut To Slim by Lindsay S. Nixon), self control, and grace to conquer? When Arnold models his body does he not deserve to be proud of his efforts? Perhaps without self control and suffering Arnold's genes would have produced perfect muscles in spite of a Twinkie addiction and laziness. I view Ozempic as equivalent to long term opiate substitution because there is no expectation to ever quit.
Drugs Are Cool
I know how cool drugs can be. Drugs may provide money or status for dealers and comfort or adventure for users. For many there is a draw to be part of the drug scene. I am drawn to this topic. Many have become volunteers, counselors, and advocates and of those many adopt the harm-reduction platform . Many have pure hearts but are ignorant of the larger agenda. Some profess themselves to be psychonauts or shamans and they can be dangerous because they glorify and promote drug use. Is it surprising to find them involved in the “harm-reduction” movement also? For them drugs are not a means to an end but the end itself. They refuse to outgrow the drugs.
I’ve discovered a lot about myself and reality getting high on hallucinogenics. I believe they were beneficial for me so I don’t absolutely condemn them but I am very weary and ultra-critical.
I endorse Timothy Alberino’s perspective;

Many others have moved past drug abuse but still find a way to be involved. Bunkpolice founder Adam Auctor developed drug testing, undoubtedly his pet project has saved many lives and raised black-market quality. “I have been a bit of a drug nerd for several years, not taking them, just studying user reports and evaluations online out of curiosity.” FI 244
Woke-Hate of Western Civilization
Fentanyl addiction does not exist in a vacuum. Practically all drug advocates are quick to point out racial disparities or systematic injustice. The issue with generalizations or deconstructionism as the only means of evaluating issues is the ease in which the default consensus is arrived at blaming capitalism or colonialism or white christian propertied males. This is a non-starter for finding solutions and in many respects it is blaming the victims.
Volkow replies:
(The Fentanyl Crisis Rages On | Talking Feds Podcast, Talking Feds with Harry Litman, 12/25/2023)
(Ep. 2: The Fentanyl Treatment Keeping People High, Discovery Institute,5/29/2024)
“Our destinies today are determined by Fates known as Capitalism, Prohibition, Colonialism, White Supremacy, and Patriarchy”. OO90
Class is a far more productive category in which to view societal disparities. Harm reduction advocates want to de-stigmatize drug abuse and remove guilt from users but primarily they spread an ideology which is founded on hate and segregation of one very specific group and worldview.
“Instead the real purpose of identity politics is to derail a class-based movement bent on radical change.” [Introduction] I’ll Burn That Bridge When I get There, Norman Finkelstein
Carlyn promotes herself as an intellectual representative for the harm-reduction cause. There are very few published books on this topic and so she is a valid target. Let me highlight her hatred of [white supremacist-colonial-capitalist males]. Of course being Jewish and female herself she is above criticism and because she has a chronic pain condition she views herself as a peer among the most oppressed. I presume she is also self-appointed to represent cobalt miners and coffee bean pickers and child prostitutes as well. Just as unnecessary as you view my need to include this issue, it is equally unnecessary for her and her ilk. This is a perfect example of conflating issues so that nothing can get accomplished other than uniting in hate against one group of people.
From Johann Hari’s history of the war on drugs in his 2015 book Chasing the Scream, she learned that there has always been a tight connection between race relations and drug war policies, that human rights of drug users are routinely violated, that it’s not just that people who use drugs are burdened with dependence on a dangerous substance, but that the substance is dangerous in large part because they are alienated from families and communities by criminalization or terrible treatment regimens or poverty or shame.” OO 102
I do agree the history of prohibition may in fact be racist but what exactly do we need to overturn? The ideal of equality before the law? Property ownership? Rather than “upend the current structures of power” I advocate a return back to those values we all cherish and leave behind those we don’t. Carolyn fullheartedly seeks to destroy but demonstrates no concept of the historical significance of our culture and rights.
“John Adams pointed out the strong features of the British constitution and praised its many excellencies. Even Samuel Adams was on record as having strongly endorsed the English system: “In none that I have ever met with this power of the governors and the rights of the governed more nicely adjusted, or the power which is necessary in the very nature of government to be entrusted in the hands of some, by wiser checks prevented from growing exorbitant.” The colonists wished to show that they were not at all in opposition to the British constitution, but only to its abuse by inscrupulous and designing men. There position was, that if the constitution were only properly interpreted and applied, there would be no ground for complaint.” A history of American Political Theories, Merriam pg.70
She is in Canada writing largely about US government and my society. Instead of understanding our legal systems and correcting them (defending our rights) her motive reeks of conformism for social approval among revolutionaries.
Carolyn writes “It sounds wild-eyed and radical to blame capitalism, colonialism, and systemic racism or white supremacy for the need for opioids as well as the raging elicit market and overdose deaths. It is radical at least, in the sense that it goes to the real root of the problem.. We need to somehow convince the relatively small number or largely white, wealthy, abled, solipsistic, and male decision-makers in the world to effortlessly understand and care about the rest of us, to actively want to diminish our pain. Or we need to upend the current structures of power.” OO 196
Magical fairies are going to manufacture and distribute full-agonists to drug abusers for life as soon as we upend the current structures of power! Instead of empowering addicts by holding them to their duty for responsible citizenship, Carolyn blames the usual villains of “systemic injustice” simply to make excuses for harm-reduction and drug abuse.
Race
Using Norman Finkelstein’s example about women I can explain how I feel about the current state of black Americans; there academic record (Edwin Black exposes IQ tests as eugenic; “the tests were vehicles of cultural exclusion” War Against The Weak pg.82) and their increased representation as criminals. I am not making excuses for poor personal choices but I do acknowledge societies influence on this group of people. I reject steep, inherently violent, punitive measures for victimless drug crimes. The police may have targeted blacks because they were already oppressed easy targets; perhaps not because they hate blacks but because they are easily identifiable prey, just as poor whites are compared to affluent ones. If blacks are poor for whatever reasons it makes them more likely to resort to crime or drug dealing for survival. This will increase across the whole population as the US middle class is progressively destroyed. The drug war further destroyed their families, communities, and economic opportunities. Poverty is the leading contributor of crime, it doesn’t help there is an ongoing state-sponsored culture-war which targets tradition and promotes racial conflict.
“John Stewart Mill asserted the full intellectual equality of women. If history recorded so few female geniuses, he maintained, it wasn’t because they had been overlooked by sexist gatekeepers but rather because in the distant past, when “great and fruitful new truths could be arrived at by mere force of genius, with little precious study and accumulation of knowledge,” women had been banished from the life of the mind, while in his day, as women were just entering intellectual domains, genius required mastery of the accumulated knowledge of the ages:
“nearly all the thoughts which can be reached by mere strength of original faculties, have long since been arrived at; and originality, in any high sense of the word, is now scarcely ever attained but by minds which have undergone elaborate disciple, and are deeply versed in the results of precious thinking….every fresh stone in the edifice has now to be placed on the top of so many others, that a long process of climbing, and of carrying up materials, has to be gone through by whoever aspires to take a share in the present stage of work…. When women have had the preparation which all men now require to be eminently original, it will be time enough to begin judging by experience of their capacity for originality. (The Subjection of Women.)” I’ll Burn That Bridge When I Get To It, Finkelstein pg. 17
In my opinion, even if specific genes made anyone “better” in any way it doesn’t matter now because there is so much wasted potential across cultures that I believe, with few exceptions and certainly not racial exceptions, that most everyone is a loser!
Carlyn like so many harm-reduction advocates, some with pure intentions, fully adopt woke far-left political views. In case you think I am speaking hyperbolically lets look at Australia’s harm-reduction goals. These are the harm-reductionists, it appears they are more transparent about their IDEOLOGY in Australia.

Is my commentary even necessary?
*
Carlyn is correct to remind us that many live with pain and suffering. She is so blinded by her hatred of conservative values she fails to acknowledge our government’s and their billionaire counterpart’s target all citizens. Her woke rhetoric is intended to fuel internal strife instead of solidarity while she believes she is above reproach. Her ideology only seeks unity against a specific group of people. Under the guise of those who have been historically oppressed she makes excuses for her cause which in reality is an entire global government bio surveillance tool-kit with no respect for local sovereignty or self determination.
Carlyn goes so far as to diminish the needs of genuine pain sufferers by conflating their needs with those of general addicts. This is not only counter productive but subversive. The outcome is nothing more than building alliances to further promote the agenda; it is hijacking. She diminishes the purpose of the group under the pretense of inclusion! By her standard, groups are not allowed to form around special interests unless their primary mission is to unite against [white supremacist-colonial-capitalist males]. She completely hijacked this online pain group and started shaming them for not being woke… she accuses them of “punching down”.
“pain patients frustrated at the change in the status … seek to distinguish themselves from the “addicts”...”drawing a distinction that reflects outrage at the suggestion that pain patients do not in fact take our medications precisely as prescribed, but which also reflects the belief that people who use illicit opioids do so to reach a state of blissful intoxication for recreational, and thus morally indefensible, purposes.”...“where our use of opioids is measured, careful, rule-following and instrumental, she implies theirs is adherent, out of control, self-indulgent, and inevitable destructive. We are being treated as junkies , those pain patients say. It’s not fair. It’s not right. But a better argument would be that no one should be treated the way “junkies” are routinely treated.”… “It dawned on me,” Lelena writes, “that Patients Not Addicts was just AWFUL after I realized how loaded it was to say that WE were patients, but folks with with Addiction weren’t. OO 191 192
Conflating issues is so common it may in fact be a tactic to ensure no solutions can ever be implemented. Carolyn (and Lelena) can’t see outside of her own conditioning. The group was formed to fight for pain-patient’s right to access medication not equality between pain patients and street addicts. Carlyn injected her woke venom which I speculate in some ways splintered and paralyzed this advocacy group. She cut off her nose to spite her face to defend her love of opioids as an addict instead of as a patient.
Carolyn misleads her readers to defend fentanyl:
“If the drugs were tested for purity and composition, this risk could be lowered to something closer to the risks involved in medical use of fentanyl in a hospital setting, which are negligible.” OO 263
In general I agree with her position except there is a serious caveat in comparing hospital use and street use:
(.429)OUPC 2023: OAT in the time of fentanyl, CAMH Professionals Videos, 4/21/2024
(Cole 2k Blues In 48 Hours, Lost in Phoenix, 6/26/2024)x2
Pain
“Mi pintura lleva con ella el mensaje del dolor”
My painting carries with it the message of pain Frita Kahlo
“Opioids can cause death: no doubt about it. But for some of us, their role is irreplaceable: striking that delicate balance-not just a life, but a life worth living, one that makes us choose to stay alive.” OO 143
“A drug that works best when I take it least often is not going to be a great solution to lifelong pain,..” OO 68
“Among older adults, the prevalence of chronic pain is more than 40%. Given the prevalence of chronic pain and its often disabling effects, it is not surprising that opioid analgesics are now the most commonly prescribed class of medications in the United States”
“A systemic review of various studies may demonstrate pretty well that, say, an opioid is not superior to an anti-inflammatory for osteoarthritis of the knee” OO 164
“Pain acceptance, as a concept hinges on the assumption that patients who, despite learning the techniques intended to promote a curious, non judgmental attitude to pain, still see their pain as “suffering”, are fighting against the idea that their pain is indeed intractable.” OO 253
“Have you ever made a plan?… The intake psychiatrist turns back to his screen and types, “She endorses passive suicidal thoughts.” And, “She is capable of caring for herself and is not an imminent risk of serious self-harm.” He sends me out the door with a list of mindfulness mediation programs to contact, recommendations that I look into mood stabilizers and anti depressants, a referral for magnetic deep brain stimulation.” OO 69
“Some doctors speak of pain sufferers principally as “difficult patients” who need to be redirected, spoken firmly to, or appeased. Others talk about the “pain lobby” a vague reference to overbearing drug marketers in cahoots with lily-livered legislators and pushover docs, along with dismissive, blindingly privileged, loose or selective with evidence, and patronizing, even as they raise valid questions about these drugs and how they are used. “ OO 52
“Today, arthritis pain is one of the principal ailments driving people to use opioids. An aging population subject to osteoarthritis- as well as higher rates of chronic inflammatory diseases like rheumatoid arthritis or AS- is going to be a population with ever higher rates of daily, maddening join pain. That’s without even considering the impact of a trend toward precarious, literally back- breaking work and unaffordable preventative healthcare upon the prevalence of back pain and other pain conditions. According to NIDA, “the bulk of American patients who need relief from persistent , moderate- to severe non-cancer pain have back pain conditions (approx. 38 million) or osteoarthritis (approx. 17 mil).” OO 56
There is almost no one who has not heard the evil pharmaceutical companies and gullible doctors conspired to hook tens of thousands of patients on opioids. Some of the collusion has been proven in court, and certainly the tactics used to promote opioid painkillers were calculating and atrocious. The backlash, though, has been reckless, moralistic, and equally loose with the truth. Increasingly, patients are scared to use the drugs after surgery, fearing that they, too , will become “hooked”. And the rhetoric around chronic opioid therapy for intractable pain has moved from “they’re dangerous” to they’re instantly addictive” to “they don’t work anyway” to “accept your pain”. OO 163
The State of Pennsylvania has set up an online form for anonymous reports of prescription drug abuse. Patients across the United States have been forced to consent to invasive, poorly evidenced procedures and treatments like spinal epidurals, high doses of steroids, ketamine infusions, or new (and just as dangerous) drug regimens as an alternative or requirement to be allowed to take opioids. that they already know work for them.” OO 131
*
“the evidence showed that acetaminophen and ibuprofen are as effective as opioids in the short term and that almost everything is better in the long run than opioids, once we take into account tolerance and the harms caused by chronic opioid use. A study from emergency rooms in New York City further blew apart our conception of opioids. Patients with acute pain were chosen randomly to get either acetaminophen plus ibuprofen, which don’t contain opioids., or a Percocet, Tylenol 3, or Vicodin tablet, which do. They didn’t know what they were given. Two hours later, they were asked about their pain. All the patients had experienced considerable and almost identical improvement in their pain” AF 109
“there was no good scientific evidence that using opioids for longer than six weeks actually helps with pain. In fact several studies have showed that use of opioids for chronic pain may actually worsen pain and functioning, possibly by potentiating pain perception…. The authors of the CDC guidelines, in conjunction with Nora Volkow, then responded by releasing more guidance on how to manage pain in a world of fewer opioids. Their alternative treatments for chronic pain included cognitive behavioral therapy, exercise, and yoga, as well as acetaminophen, ibuprofen, and other classes of medication. They pointed out that anti-inflammatory drugs such as ibuprofen and naproxen are first-line medications for both osteoarthritis and low back pain, two of the most common reasons for opioid prescriptions in recent decades.” AF 111
“In March 1996 the makers of the top two products in the 2.7 billion over-the-counter painkiller market, Tylenol (acetaminophen) and Advil (ibuprofen), starting an ad war over side effects… McNeil's ads warned people who have ulcers or take blood pressure-lowering medicines that ibuprofen could be dangerous… In February 1996 [Whitehall-Robins] the company began running ads warning those who drank regularly to consult their doctors before taking Tylenol.” BP 303
WHO guideline for non-surgical management of chronic primary low back pain in adults in primary and community care settings
https://www.who.int/publications/i/item/9789240081789
If you are simply trying to use less opioids why would you ignore natural and less dangerous solutions. In this document WHO rejects arnica, ginger, topical white lily, and… Topical combination herbal compress [Zingiber cassumunar Roxb. rhizomes, Curcuma longa L. rhizomes, Cymbopogon citratus (DC.), Stapf leaves and leaf sheaths, Croton roxburghii N.P.Balakr. leaves, Tamarindus indica L. leaves, Citrus hystrix DC. peels, Blumea balsamifera (L.) DC. leaves, Vitex trifolia L. leaves and camphor] and WHO also rejects: Topical combination transdermal diffusional patch [Oleum thymi, Oleum limonis, Oleum nigra, Oleum rosmarini, Oleum chamomilla and Oleum lauri expressum]
Unlike the CDC Clinical Practice Guideline for Prescribing Opioids for Pain — United States, 2022 of which The recommendations do not apply to pain related to sickle cell disease or cancer or to patients receiving palliative or end-of-life care. The WHO guideline for non-surgical management of chronic primary low back pain in adults in primary and community care settings specifically opposes opioid use for chronic pain.
I claim WHO simply want to ignore plant medicines because they are effective. They write their back pain guide as if every patient will recover from pain but some people will have to live with pain for the rest of their lives. They admit nsaids are for short term use. Don’t forget boswelia, wild lettuce, tumeric, and of course kratom. The WHO promotes nsaids despite well documented risks while ignoring plant medicines given the absence of sufficient evidence to judge the balance of benefits and harms. I include their detailed “blacklist” for obvious reasons. If your struggling with these issues I would look over this document as they also reject injectable local anaesthetics and Glucocorticoids and also includes a section on Physical interventions: Structured exercise therapies or programmes, Needling therapies (traditional Chinese medicine acupuncture and other dry needling modalities), Spinal manipulative therapy, Massage, Traction, Therapeutic ultrasound, Transcutaneous electrical nerve stimulation, and Assistive products: lumbar braces, belts and/or supports and mobility assistive products.
I don’t wish to diminish the value of opioids for pain management. I don’t believe the establishments claims that opioids aren’t effective long term; if you use them strategically they may enable you to live instead of merely survive. Carlyn’s entire book is foremost a tribute to tramadol which allows her to function given her chronic condition. But like many issues, patient self reporting of pain solely relies on subjective criteria; like depression, there is no way to quantify pain. Exactly how crazy am I? ADHD also has no objective criteria yet there are plenty of diagnoses. Netflix has a two part video series called Take Your Pills, one of which is about Adderall, I recommend them both.
Volkow most often diminishes behavioral and societal factors and instead blames our genes (as do eugenicists and racists); “genetic vulnerability accounts for at least 35 to 40% of the risk associated with addiction, and that adolescents are at increased risk because of the enhanced neuroplasticity of their brains and their underdeveloped frontal cortex.” Misconceptions 2016
Children are vulnerable, she knows this, but does she raise objections to over prescribing Adderall to 4 year old children? I suspect not because a reductionist worldview is what is used to justify ADHD prescriptions.
Suicide
“In Oregon, restrictive prescribing- for the poor, anyway- reached a point where opioids were to be banned for all chronic pain patients on Medicaid, with no new starts on the medicine and with even existing, stable patients tapered to zero. OO 130
“The DEA has raided numerous doctors’ offices, sometimes entrapping physicians by faking a medical condition. And not just the small number who really have something shady going on, but respected physicians who treat patients no one else will take- patients who, after finally finding stability through a steady healthcare relationship and an effective, tolerable dose of opioids., lose access to both physician and drug, plunging every aspect of their lives in chaos. Even in those cases, certainly real, where doctors are dispensing pills with non intention of actually treating pain, or who are prescribing in dangerous amounts or ways, prosecutions have left hundreds, sometimes thousands of patients with a physician. Apparently, no one has stopped to consider or care what happens to the real pain patients in these situations… Doctor’s in turn, abandon high-needs pain patients because of the risk of prosecution, increasingly onerous paperwork and reporting requirements, and disciplinary action if they are thought to be prescribing too many opioids. Prescription monitoring databases, again intended to prevent double-doctoring or prescription diversion to the illicit market- and, more importantly, to help pharmacists work with doctors to alert patients to possible dangerous combinations- are instead being used punitively, with information shared with law enforcement and the DEA, and patients unnecessarily humiliated with urine tests and pill counts. The State of Pennsylvania has set up an online form for anonymous reports of prescription drug abuse. Patients across the United States have been forced to consent to invasive, poorly evidenced procedures and treatments like spinal epidurals, high doses of steroids, ketamine infusions, or new (and just as dangerous) drug regimens as an alternative or requirement to be allowed to take opioids. that they already know work for them.” OO 131
“Dr. Kertesz has been keenly aware of the need for hard evidence. At last, he, along with other colleagues, published an observational study in the BMJ that looked at 1,394,102 veterans who had been tapered or cut off their prescribed opioid painkillers between October 2012 and September 2014. Over that time period, there were 2,887 deaths due to either overdose or suicide. Stopping opioids treatment was thus associated with a significant increased risk of death from overdose or suicide.” OO 133
“Kertesz says “What concerns me even more is how little we understand, or even seek to understand, about why they happen.” Not until we were four years into the unintended consequences of the 2016 guidelines did the CDC produce a docket on pain and opioids that finally included mention of publicly reported deaths due to suicide.” OO 134
“Thousands of private practices, hospitals, insurance providers, and clinics continue to cite the CDC as the reason they are cutting off their patients, lowering effective does, subjecting their patients to drug testing and pain contracts, even abandoned patients, leaving hundreds of thousands of sick, vulnerable, and disabled people without any healthcare at all.” OO 134
While until recently in North America, opioids were prescribed loosely and often where other treatments were more appropriate, elsewhere the problem has been not of a glut but of a lack of opioids and a lack of access to them. This global imbalance is exacerbated caused, in fact- by the US-led war on drugs, which puts pressure on countries to permit less opioid importation than they in fact need to supply legal painkillers to their citizens… [In 2016 there were new] US guidelines for opioid prescribing for chronic pain by the CDC. These have spurred a rapid, dramatic, and poorly- thought- out crack down on opioid prescribing that has left individual patients in these countries in preventable pain as well. .. The CDC’s guidelines were intended to reduce inappropriate prescribing (that is, use of opioids when an alternative would do, or when the harms to an individual patient outweigh the observable benefits). But across the US, they have been re-interpreted by local health organizations, other quality and standards bodies, government departments, and insurance providers as a warning that opioids are not indicated for chronic pain at all.” OO 129-130
“As part of it’s war on drugs, the DEA limits the supply of opioids that can be imported into the US. Tighter restrictions mean fewer drugs available to treat addiction and chronic pain, but also fewer for patients on ventilators, for patients in or after surgery, for women in labour, for cancer patients, for those on their way out. OO 142
“Retired Cpl. Christine Gauthier, who has been trying to get a wheelchair ramp installed at her home for the past five years, testified on Thursday that a caseworker told her that they could give her assisted dying, even offering to supply the MAID equipment for her.”
"It was just getting too much and unbearable. And the person at VAC mentioned at that point, 'Well, you know that we can assist you with assisted dying now if you'd like.' And I was just shocked because I was like, 'Are you serious?' Like that easy, you're going to be helping me to die but you won't help me to live?" she said.
Paralympian trying to get wheelchair ramp says Veterans Affairs employee offered her assisted dying, Tom Yun, CTVNews, 12-3-22
“There is a very real risk of their lives being considered “not worth living,” and of disabled people thus being nudged toward their own deaths, or of poor and disabled or mentally ill people being denied the supports- anything from adequate income to morphine to accessible housing- they need to achieve an adequate quality of life, and instead resorting to this form of euthanasia for lack of other options.” OO 140
True to course, harm-reductionists also promote euthanasia.
“Maier-Clayton, who suffered from depression and obsessive thoughts as a child, also (as an adult) experienced burning, acid-like pain from what was diagnosed to be the result of Somatic Symptom Disorder, a psychiatric condition. He received endless hours of psychotherapy, and antidepressants. Maier-Clayton became a right-to-die activist who advocated for the expansion of eligibility for newly legal doctor-assisted suicide. He wanted the option to apply to people who felt they no longer wanted to live due to depression or other mental illness, or due to intractable pain.” OO 139
Child Euthanasia without Parent Approval Pushed for Canada, By Wesley J. Smith, October 2, 2018
Dan Dicks summarized this movement; Death Capsule Deemed The “Tesla of Euthanasia” To Be Used For The First Time later This Month!!, Press For Truth, July 5, 2024
https://odysee.com/@PressForTruth:4/Sarco-Death-Capsule:d
Can we infer euthanasia falls under harm-reduction
Reuters fact checkers couldn’t even cover for Bill Gates. You would think a team of woke PHD’s could do better than this:
“First, we've got population,” he said during the talk organized by TED, a non-profit organization devoted to spreading ideas. “The world today has 6.8 billion people. That's headed up to about nine billion. Now, if we do a really great job on new vaccines, health care, reproductive health services, we could lower that by, perhaps, 10 or 15 percent. But there, we see an increase of about 1.3.”
However, Gates was not suggesting the global population should be killed off using vaccines. He is instead saying that improving public health using vaccinations can reduce unsustainable population growth in the future – and with it, lower carbon emissions.
The Microsoft co-founder has long been a proponent of population control to target the roots of poverty and unrest.
In 2011, he told Forbes magazine that when he first entered public health it was to focus on contraception. Bill Gates quote about vaccines and population growth has been taken out of context again, By Reuters Fact Check, April 22, 2021
Government looked Left
“The WHO then planted the poisoned seed: freedom from pain is a universal human right. This eventually led to the idea that denying a patient opioids or an increased dose of opioids violated that right” AF 42
[Anna Lembke] traced it to the impetus to treat pain regardless of other considerations, arguing that ‘self reports of pain are above question, and the treatment of pain is held up as the holy grail of compassionate medical care.”.. Patient satisfaction surveys included pain management ratings, and physicians who were reluctant to give opioids would receive poor ratings that could affect their income and job security.” AF 77
Micke Brown told the hearing that patient registries were punitive and “further stigmatize people with pain, create additional hardships, and erect new barriers to effective pain care” AO 172
The Pain Care forum and American Pain Foundation fell back on the tested strategy of claiming that the REMS proposals threatened treatment for million of people who should not have to suffer because of drug addicts.. it gathered thousands of signatures for a petition opposing a patient registry. The APF called on the FDA to protect the rights of people with pain.” AO 171
BDM (Brain Disease Model of Addiction)
(Zoloft)
This issue is not new, this is written in 1999; At that time, NAMI (National Alliance for the Mentally Ill) was a loose confederation of local self-help groups for parents of schizophrenics. Its main goal. Besides providing shoulders for each other to cry on, was to convince psychiatrists that bad parenting did not cause schizophrenia, and good parenting alone couldn't cure it. At the time, this was an open debate… One of NAMI’s biggest political weapons has always been pills, which it jams down peoples throats, figuratively and, in the view of some, literally. If symptoms can be checked by medication, the group argues, very loudly, then serious mental illnesses are biological, not psychological: “not out fault”. This admittedly reductionist position is meant to help destigmatize serious mental illnesses for people who have them, treat them and study them. It has also been a perfect way to get the right people on NAMI’s side… For many years, there was little downside to NAMI and the drug companies being on the same side because they were both selling the same product: biological psychiatry. BP 164
“Ironically, the brain disease model's ascendance in the U.S. corresponds with epidemic rises in opiate addiction,” People Control Their Addictions, Stanton Peele
“we need to treat addiction as a medical challenge, not as a moral failing” Alex Azar, FI 237
“The brain disease model of addiction is less stigmatizing than the view of addiction as a moral failing, and it brings hope that medications can be developed to address the disease. There is strong evidence supporting this paradigm, with neuroscientific research pointing to observable brain changes” https://www.hazeldenbettyford.org/research-studies/addiction-research/brain-disease-model
“The goal of the brain disease model of addiction is to remove any idea of the drinker or drug user as an active participant in their recovery, as someone capable of enacting an intention to quit in line with their values (see Peele, 1987a). Instead, this model sees humans as biological automatons who must rely on—can only be passive recipients of some modern medical miracle, a la NTX, that isolates and removes the neurochemical source of their addiction.” People Control Their Addiction, Stanton Peele
“In summary, addiction as the idea that people are irresistibly, inexorably, irreversibly stuck in a drug dependence so that no effort of will can extricate them is wrong, as proved by research that directly tests this belief. Yet Volkow has no fear of being contradicted while claiming the counterfactual assertion and, moreover, cloaking it with the mantle of science.” People Control Their Addiction, Stanton Peele
Brain Disease Model advocates claim all relevant data falls within their own specialized domain subjecting all evidence solely to their own interpretation and rendering their conclusions and extrapolations beyond criticism.
“There is some experiential configuration that creates both the addiction and change that can't be broken down into neurochemical, cognitive, and situational components. The residue strongly resembles what might be called free will (Peele and Thompson, 2015).
Therapy is often directed to lowering a person like this woman's anxiety levels and to figuring out her experiential and situational keys—called addictive cues or triggers—for the purpose of assisting her to abstain. But it's the woman's right to refuse to participate in this process, and our obligation to accept her choice. What is wrong, and immoral, is to tell the woman that such change isn't possible. This phenomenon of mislabeling continued addiction as a biological imperative has been embedded in harm reduction by Dole and Nyswander (1967), the developers of methadone maintenance, through their claim that former heroin users absolutely require substitute narcotics such as methadone or buprenorphine because they suffer from a permanent “metabolic disease.”People Control Their Addiction, Stanton Peele
Using the paradigm of Wayne Skinner, co-author and social worker in Toronto “addiction may be viewed as a brain disease, or as a moral failing, or as a “disease” of choice, or as a life sentence meted out in one’s genes.” OO 54
The disease model suggests that addiction is a diagnosable disease similar to cancer or diabetes. This model attributes addiction to a chemical imbalance in an individual's brain that could be caused by genetics or environmental factors. The second model is the choice model of addiction, which holds that addiction is a result of voluntary actions rather than some dysfunction of the brain. Through this model, addiction is viewed as a choice and is studied through components of the brain such as reward, stress, and memory. Addiction Psychology, Wikipedia
“The initial decision to take drugs is typically voluntary. Brain imaging studies of people with addiction show physical changes in areas of the brain that are critical to judgment, decision-making, learning and memory, and behavior control..Scientists estimate that genes, including the effects environmental factors have on a person's gene expression, called epigenetics, account for between 40 and 60 percent of a person's risk of addiction.. Although taking drugs at any age can lead to addiction, research shows that the earlier people begin to use drugs, the more likely they are to develop serious problems. It also may result from a mix of early social and biological risk factors, including lack of a stable home or family, exposure to physical or sexual abuse, genes, or mental illness.” Drug Misuse and Addiction, https://nida.nih.gov/publications/
In addition to the neurobiological changes, the brain disease model of addiction also notes that many genetic, environmental and social factors contribute to an individual's vulnerability to begin using drugs, to continue using drugs and to undergo the progressive changes in the brain that characterize addiction. Butler Center for Research May 2021
“The disease model of addiction describes an addiction as a disease with biological, neurological, genetic, and environmental sources of origin...The contemporary medical model attributes addiction, in part, to changes in the brain's mesolimbic pathway ” Disease model of addiction Wikipedia
This is a strategic lie, the BDM diminishes environmental or sociatal factors: “Understanding the impact that genes, reward, memory, stress, and choice have on an individual will begin to explain the Disease Model of Addiction” “Addiction Psychology” Wikipedia
1.Genetic- closely tied to (chemical-imbalance), both outside our individual control and only within the domain of “experts”
2.Reward- is based on dopamine
3.Memory- is centered around the neurochemical [glutamate]
4.Stress- is based on brain chemistry and “allostatis”
5. Choice- revolves around damage to the orbitofrontal cortex (OFC), the anterior cingulate cortex (ACC), and the prefrontal cortex (PFC)
(Don’t be fooled by the word “choice”, the choice-model is something else, popularized by Gene Heyman)
“The biological mechanisms typically claimed to underlie all forms of addiction (CREB and ΔFosB) — while psychosocial factors are considered as only tangential issues leading to lesser or greater use and exposure...” Life-process model of addiction Wikipedia
*
The brain disease model of addiction: is it supported by the evidence and has it delivered on its promises? The Lancet, January 2015, Hall, Carter, Forlini,
We critically assess claims about the medical and social benefits of use of the BDMA because the social implications are often implied as a reason to accept this model.
Furthermore, we argue that the BDMA is not supported by animal and neuroimaging evidence to the extent its advocates suggest; it has not helped to deliver more effective treatments for addiction. The focus of the BDMA is on disordered neurobiology in a minority of severely addicted individuals, which undermines the implementation of effective and cost-effective policies at the population level
to discourage people from smoking tobacco and drinking heavily. The pursuit of high technology direct brain interventions to cure addiction when most individuals with addiction do not have access to effective psycho-social and drug treatments is questionable.”
Leshner acknowledged that drug use was initially voluntary,...he argued on the basis of animal models that chronic drug use flicked a neurochemical switch in the brain, making it very difficult for people addicted to drugs to stop using them… they argue that the results explain how chronic drug use hijacks the brain's reward systems.
Proponents of the brain disease model of addiction (BDMA) have been very influential in setting the funding priorities of NIDA, and by extension the bulk of publically supported research on addiction. In 1998, Leshner testified that NIDA supports more than 85% of the world's research on drug abuse and addiction.
An increased acceptance of the BDMA is also predicted to reduce the stigma associated with drug addiction by replacing the commonly held notion that people with drug addiction are weak or bad with a more scientific viewpoint that depicts them as having a brain disease that needs medical treatment.
The BDMA is not co-extensive with neuroscience-based explanations of addiction.
Critics of BDMA contest claims by its proponents that addiction is a chronic relapsing disorder and cite epidemiological evidence that most people with addiction recover without treatment
Leshner predicted the BDMA would help to develop drugs and behavioral treatments to reverse or compensate for the brain changes underlying addiction, thereby delivering more effective treatment for addiction. New drugs to treat addiction include vaccines and implantable agonists and
antagonists against neurotransmitters to decrease the risk of relapse; DNA tests to match patients to the most effective treatment; drugs to modulate the stress response; drugs to modify memories of drug-related…
Considerable scientific value exists in the research into the neurobiology and genetics of addiction, but this research does not justify the simplified BDMA that dominates discourse about addiction in the USA and, increasingly, elsewhere. Editors of Nature were mistaken in their assumption that the BDMA represents the consensus view in the addictions specialty, as shown by a letter signed by 94 addiction researchers and clinicians (including one of the authors of this Personal View).”
*
“The pursuit of high technology direct brain interventions to cure addiction when most individuals with addiction do not have access to effective psycho-social and drug treatments is questionable.”
“One such intervention is called a NSS-2 bridge device”
“The goal of these studies which aim to explicate the molecular and cellular basis of drug addiction is to eventually develop biologically based diagnostic tests, as well as more effective treatments for addiction disorders.” Cellular basis of memory for addiction, Eric J. Nestler
I wonder if it’s a coincidence? This seems like the same brain-implant agenda of Elon Musk! Are Volkow and Musk working for the same ends?
Volkow gives us a citation; her entire worldview, whatever she’s arguing for is based on this study: “As discussed above, study of the direct involvement of synaptic plasticity in development of opioid addiction is very much in its infancy Systems-level adaptations are complex and still poorly understood but could provide important therapeutic opportunities if the suggestion that astroglial activation plays a role in opioid tolerance and withdrawal, and perhaps synaptic plasticity through cytokine production, proves to be important in opioid addiction.” Cellular neuroadaptations to chronic opioids: tolerance, withdrawal and addiction, M J Christie
“The person who has had a cocaine use disorder has lower levels of the D2 dopamine receptor.” And this has to do with the price of corn, how? Keep your eye on the proposed solutions “ important therapeutic opportunities”. These solutions are why billionaires subscribe to this scientism, they don’t care about addicts’ well being but instead use their plight as an excuse to deploy bio-surveillance medical intervention technologies. But I’m sure Trostky’s granddaughter, Nora Volkow, leaves her biases at the door.
Here is another of very few examples for reference;
For example, scientists recently performed a genome-wide association study to try to identify genes that might put people at risk for problematic cannabis use. They identified a genetic locus on chromosome 8 that controls the levels of the gene CHRNA2 expressed in the brain. Low levels of expression of the gene CHRNA2 in the cerebellum are found to be associated with cannabis use disorder, including diagnosis at an earlier age. The findings suggest that under-expression of CHRNA2 in the cerebellum (and probably other brain regions) is involved in cannabis use disorders, and provides a potential target for future prevention strategies, therapies and medication. Research Update, Butler Center For Research May 2021, Hazelden Betty Ford
More proof that their grounds are based on incomplete science and speculation:
“drug addiction, which can be defined as the compulsive seeking and taking of drugs despite horrendous consequences or loss of control over drug use, is caused by long-lasting drug-induced changes that occur in certain brain regions. Only some individuals, however, succumb to addiction in the face of repeated drug exposure, while others are capable of using a drug casually and escaping an addiction syndrome. Genetic factors account for roughly 50% of this individual variability in addiction vulnerability, and this degree of heritability holds true for all major classes of addictive drugs, including stimulants, opiates, alcohol, nicotine, and cannabinoids. It has not yet been possible to identify most of the genes that comprise this genetic risk, likely due to the involvement of perhaps hundreds of genetic variations summating in a single individual to confer addiction vulnerability”...” Finally, efforts to understand the molecular-cellular mechanisms of memories related to addiction find themselves at the point at which all other efforts to understand the biological basis of behavioral memory now struggle: our ability to relate biological phenomena to complex behavioral memory remains extremely difficult. Overcoming this divide represents perhaps the greatest challenge in the neurosciences. Cellular basis of memory for addiction,” Eric J. Nestler
Volkow’s prerogative is more important to her than an accurate presentation of the facts alone. In my opinion her solutions based on the BDM will amount to invasive and controversial medical procedures.
The stage is already set to deny addicts self autonomy or in other words consent. Is it a surprise “consent” itself is the recent issue? FDA eases informed consent requirements for minimal risk trails, Regulatory News Dec. 21 2023
Choice
So.. “initial drug use is voluntary”. In our society, by adulthood, we know that illicit drug use is a crime. Despite arguments based on libertine ideals and abstract freedoms, drug use has historically been viewed as morally wrong. It is also common knowledge that illicit drugs are often contaminated and drugs hinder self control and can make us freak-out depending on the drug, its potency and dosage, or unknown contaminates. Where is the accountability for the wrong of initial drug use and the reoccurring use that solidified the addiction? Are addicts victims?
Gene Heyman (2013), analyzed the most recent NESARC data according to a timeline of likelihood of quitting a drug dependence: Using this Times case in a workshop, I said: “Well, of course, this therapist did a brain scan to show that this particular woman has a particular neurochemical reaction proving nicotine has the key to her brain.” No she (the therapist) didn't. She wouldn't know how. Nobody does. There is no such neurochemical key. Nor can a brain scan show that people are able, or on the verge, of quitting or cutting back their addiction. There is some experiential configuration that creates both the addiction and change that can't be broken down into neurochemical, cognitive, and situational components. The residue strongly resembles what might be called free will,” People Control Their Addictions, Stanton Peele
Safe Supply
“, buprenorphine increasingly promoted as an alternative to other opioids for chronic pain patients because it is thought to have less risk of addiction (because of its lower “likability”), is a lifesaver for those at high risk of overdose. But for some people, likability is the essential factor in being able to stick with a treatment, and without a substance with high likability they are simply unable to function in their lives.” OO 271
Likability matters for criminals; This is yet another shallow excuse to defend continued illicit drug abuse. Carolyn wants to coddle and cater to recreational drug addicts, perhaps she should burp them too! Perhaps jail sentences should also be accommodating and pleasant lest we not like them! I do not endorse a punishment model for drug addiction (as Carlyn claims of Volkow later), but I promote interventions which are necessary and scalable. The State paints jail walls disguising colors as psychological torture; I am not advocating retribution for drug users but neither will I exert extra effort to make a criminals experience pleasant and especially at the cost of enabling their addiction. In treatment of any kind, while resources are scarce, I see no room for anything other the basic detox and taper-down plan. I was recently informed that in my local jail they give inmates caffeine powder packets in case they are addicted. A large message from my addiction research is how caffeine is a gateway drug, never mind the toxic nature of industrial derived caffeine and how extracts may be abused. I was told by an anonymous source, anonymous because their ego is larger than their will to contribute to my research, that in a specific jail they ask if you want buprenorphine regardless of a previous opioid addiction. Gateway drugs in jail; a new spin. I do recommend A Scanner Darkly, my research only reinforced the message of that movie.
(A year of drug decriminalization in B.C., The Globe and Mail ,2/8/2024)
“expand the types of medications”; medication literally means meth and fentanyl.
(powdered fentanyl .889)
“alternatives” isn’t intentionally ambiguous! Have they paralyzed you, given you cognitive dissonance by obscuring the line between MAT and safe-supply yet?
These are in the same league as buprenorphine:

MAT, which includes Opiate Substitution Therapy seamlessly degrades into safe-supply which carries another meaning which in practice amounts to free illicit drugs again with no plan for abstinence. This seems to be a deliberate conflagration of terms, nothing more than enabling and supporting the most destructive drug addictions; free pure meth and fentanyl.
(ayearin .592 4)
I had to spend a while on terms and definitions after I realized that “treatment” was not “abstinence”. What defines treatment for harm-reductionists is substitution; a legal drug for an illegal one,[they could be the same exact drug]. Let’s look at some terms to see how obfuscated our language has gotten:
“When an individual with an OUD is stable in an MAT program, he or she will experience a reduction or elimination of the symptoms that qualify them as having OUD (for example, continued intense cravings, continuing to use substances despite negative consequences, persistent desire but inability to stop substance of misuse, etc). Individuals who are engaged in agonist-based MAT (buprenorphine and methadone) report significant reduction in the aforementioned symptoms, feeling “normal” or “clear-headed,” and having an increased ability to focus on other areas of their lives… treatment to achieve better health outcomes.” An Overview of Medication-Assisted Treatment for Opioid Use Disorders for Criminal Justice-Involved Individuals Jessica Reichert, Lily Gleicher and Elizabeth Salisbury-Afshar|2017-07-18|,
Carolyn promotes any plans to make opioids more available such as Dana Larsen’s; “giving away opium poppy seeds then “crowd-sourcing” the sap”, and Fair Price Pharma, “a new company company which aims to become the country’s [Canada] first domestic producer of injectable, prescription heroin, with a medicine wonderfully named Opiax.”
I must contend the “prescription” requirement is simply red tape she does not endorse.
And PANDA- the Pan American Network of Drug-user Activists which aims to deepen the cross-continental work to address the multiple harms of prohibition and eliminate overdose (or “drug-poisoning”) deaths.” OO 301
“a partnership with Mexican farmers would allow for fair trade across borders as an alternative to the war on drugs.” OO 301
I am not a geopolitical analyst however I do know “free trade” is a weapon used to destroy local economies and sovereignty. Under the aforementioned safe-supply Carlyn is promoting Mexico produce and distribute drugs across borders. She again uses linguistic manipulations to sell her point; free trade is not fair trade. I criticize Fair Trade USA in almost every paper I write, and if you want to go deeper into the war against producers https://mattcircus.substack.com/p/modern-charity
“We expanded our insurtech portfolio and piloted an industry-first solution with blockchain-enabled smart contracts for crop insurance for smallholder farmers across Kenya
“The small producers, on the other hand, can hardly write their own name,” said Jesus Gonzales, a farmer at Tajumuco Cooperative in Guatemala.” Colleen Haight
(Matt Johnson, audio)
Questions
Post-modernism claims there is no objective Truth:
Is recreational drug use wrong?
Is addiction to drugs (used for recreation) wrong?
Is addiction a choice?
I respond; the physical state of addiction is not voluntary, but an individual can chose to fight the addiction or surrender and allow themselves to self-destruct. The choice of using, with or without a pending addiction, is a conscious decision and every decision has repercussions. Even if the legal or medical establishment tries to protect us from consequences of drug abuse, natural and divine law will inevitably exact its toll.
If addiction is not wrong/bad why treat it?
Whose responsibility is it to manage our addictions?
When do we accept responsibility for ourselves, 18? Were addicts innocent during the time of their initial drug use led to addiction? If they were minors do we excuse them now as addicted adults? Do we blame their parents? Do their parents have control of them if they are in public school? My proposition of irrevocable guilt by initial use may be unfair if they started as minors. If they can’t quit on their own without support, as adults do they not have the capacity and responsibility to seek treatment. This may seem like hypothetical quibbling but I don’t want to ignore any significant variables. I am assuming it is only a minority of addicts who are drugged against their will and they would also be excused from my finger pointing, up to the point when their freedom is recovered and they can seek treatment. Then their initial use would be excused but their continued, especially prolonged use, would be subject to my criticism.
Do addicts possess willpower to manage their own addictions?
Under what circumstances should public money be spent on those whose life decisions led into addiction?
What constitutes success? More arrests, more living users, more seizures and profits, or harsher penalties? For harm-reductionist s success may be measured in more drugs on the street and increasing the availability of drugs and paraphernalia.
(this is a very weird .890) This Is a Very Weird Moment in the History of Drug Laws, New York Times Podcasts, 5/10/2024
(Ayearin .142) A year of drug decriminalization in B.C., The Globe and Mail ,2/8/2024
This project boils down to one issue so it’s inevitable to be repeated ; When giving addicts less potent opioids (known as buprenorphine, which is a partial-agonist and safer than other opioids) many patients don’t adhere to treatment. Keep in mind that the majority passing through recovery programs don’t succeed anyway. Harm-reductionists genius solution is not only to lower the barriers to access MAT/ OAT/OST (Medically Assisted Treatment/ Opioid Agonist Therapy/Opioid Substitution Therapy) drugs but also to provide stronger drugs, even equivalents, so illicit drug users might continue the “treatment” longer. They rightfully argue that the cost of putting addicts through the health care and penal system is a greater burden than providing them drugs. Per my argument; this is an example of focusing too much on what works and because their claims may all be true with beneficial outcomes it makes my argument against safe supply difficult.
I have other arguments against trusting the State and Big Pharma to be my drug dealer.
[Abusing Oxycontin, because it was intended for pain, was wrong but today a new justification to keep users on prescription opioids even without a genuine pain need is popular! Can you imagine how much money the cartels have redirected away from the Big Pharma. Every Fentanyl addict today, upon entry into a MAT program, stands to be a lifelong customer of legal prescription opioids.]
I could argue against allowing homeless addicts to be grist for the surveillance-state. I could argue for fiscal responsibility by the State against buying recreational drugs. I could argue against rewarding bad behavior; perhaps I want the state to pay for my trade school as a reward me for not wasting my life! But my foundational argument is based on values; you decide for yourself if forming an addiction to recreational drug use is wrong and then go further and decide if the state should not only refrain from punishing this behavior but reward (I consider welfarism a reward, legally it is called a benefit) it by enabling and maintaining the drug abusers opioid addiction for life. I only believe in using substitution opioids to continually taper down to abstinence as soon as possible. Only rare exceptions require a lifelong addiction to buprenorphine. Many harm-reductionists rally against abstinence based treatment models evidencing their goal for life long addictions.
Tapering
“They don’t just want to get high; they desperately want to avoid entering the world of withdrawal. I’ve heard the state of withdrawal compared with having a plastic bag over your face, you will do anything to get it off, commit any crime.” AF 19
“Suboxone Microdosing, a method which does not require them to go through withdrawal” which I wrote about already in my previous paper is also titled; the Bernese method.
“The simplicity of this method is that it does not require patients to go into withdrawal or stop using drugs immediately. The woman was initially given a tiny dose while she continued to use heroin. After only five days, she had stopped heroin, and her buprenorphine dose was rapidly increased.” AF 95
“Researchers then gave the patients various doses of buprenophine by mouth and took more PET scans to determine how much buprenophine was needed to block the carfentanil from attaching to the brain. It turned out the dose was around sixteen milligrams, which correlates to around two to three nanoliters of buprenoohine per milliliter of blood. That target of at least 2 to 3 milliliters in the blood was then set as the target for the buprenophine treatments. AF 97
[Dr. Brodie Ramin lost his patient Darla] “Darla had to make a decision every day about how much buprenophrine to take, and every day she decided to take less and less. What if I could have made the choice easier for her by taking away her choice? [for example with monthly injections or an implantable device].. I did as she asked, hoping that the lower dose would still hold her. But as I sat in Grenwald’s lecture looking at pictures of brains lit up by radioactive carefentail, I understood why she had died. Her dose was too low to block the fentanyl powder she had injected.” AF 97-99
So overdose by way of relapse can be prevented with a minimal level of buprenorophrine in the body? But if a user doesn’t feel the effects of their illicit drug they may chose to use increasing amounts; the consequences of this I don’t know. Buprenophrine alone is branded Subutex, and it’s extended release injection is titled Sublocade.
To clarify; naltrexone also blocks those who relapse from getting high. Naltrexone, when it is taken orally is inert, so ignore the effects of naltrexone in Suboxone (it’s purpose is as a deterrent from injecting the buprenorphine). I must clarify these confusing details and drug names. If I repeat myself, sometimes it’s for your sake and other times it’s because editing is mind numbing. This report is not a thorough scientific education piece it only lays the groundwork to address the controversies.
Dr. Ramin, The Age Of Fentanyl, is against harsher penalties and against abstinence based recovery programs. He argues that safe injection sites do not promote drug use but instead connects users to services. He also believes in technocracy and vaccines, for example hoping a phone app could detect overdoses and auto inject naloxone. He wants the medical profession to not over prescribe opioids but conversely allow them to flow freely on the street.
*
Who defines the arbitrary line that relieves us of responsibility, accountability, autonomy, self-determination? When does society cater to us as victims from whence we become entitled to special privileges and welfare? Is it our first-ever or second-helping, after 5 days, 2 weeks, or 7 years that the habit turns into an “addiction” over which we have no control or accountability? The “Brain Disease model of addiction” seems to claim that once the addiction changes the brain it is no longer the addicts fault. They go further with claims of predetermination. They claim there is no ability for self-control. Here is Volkow’s direct statement:
“We can do much to reduce the shame and the stigma of drug addiction, once medical professionals, and we as a society, understand that addiction is not just ‘a disease of the brain,’ but one in which the circuits that enable us to exert free will no longer function as they should. Drugs disrupt these circuits. The person who is addicted does not choose to be addicted; it’s no longer a choice to take the drug. Addicted people in my laboratory often say it’s not even pleasurable. ‘I just cannot control it.’ Or they’ll say, ‘I have to take the drug because the distress of not taking the drug is too difficult to bear.'” Dr. Nora Volkow, Addiction Is a Disease of Free Will -https://www.breakingthecycles.com/2015/06/21/disease-of-addiction-disease-of-free-will-dr-nora-volkow/
Those who argue based on values are not often trained in neurology. Not only is advanced science needed to reject their arguments, not only do we need to unpack hard data (they sponsor) but we need rhetorical skills but not to sell our opinions but instead to detect fraud in theirs. They extrapolate from proven and valid changes in the addicts brain claims that addicts have no ability for self control (among other claims). The existence of any sober addict in any small town is proof this is ridiculous. Many agree that our brains respond to different addictions in the same way. For all of time many have found the inner strength to conquer addiction. BDM’s claims are disproven by this fact alone. This is such grand evidence it is the primary evidence against the BDM.
Harm-Reduction VS BDM
Carolyn, of whom we will spend much time criticizing, claims that “harm-reduction” is not funded. But I disagree. I must admit there is nuance she must be aware of that I have not picked up on between Brain Disease Model “scientists” and Harm reduction advocates. Generally I regard them as ideologically similar especially if harm-reductionists derive their evidence from BDM claims. Public funding undoubtedly supports the BDM. Those of my persuasion oppose harm-reduction, I don’t believe I have seen the NIDA oppose harm-reduction.
“Everyone knows that if you write the words harm reduction in a proposal [to them] it will not get funded,” says Sheila Vakharia, deputy director of the Department of Research and Academic Engagement at the Drug Policy Alliance. The bias that the American organization that funds 90 percent of research on drugs worldwide brings to its work is right there in the name: National Institute on Drug Abuse, or NIDA.” OO 275
“Drugs and addiction have been political ever since the prohibition of opium and given the influence that the American-led war on drugs has upon numerous aspects of the life and fortunes of people around the world, her role- which determines most of the research done on psychoactive drugs globally is deeply political..” Instead of abstinence, we are devising ways of treating addiction in which the individual is trained to think that the environment in which they were consuming their drugs is no longer pleasurable,” Volkow tells the Lancet. Guided by NIDA’s research and communication focus on abuse in pursuit of irresponsible pleasure, we attribute all sorts of harms to drugs that are not in fact inherent in the substances themselves. As a result, drug use in general is conflated with addiction, or disordered use, which in turn is considered to derive from problems in the individual rater than seen as one response of creative humanity to difficult circumstances- circumstances like poverty, colonization, family separation, homelessness, or racism.- that result from inherently political policy decisions. And so the response and the entire way of understanding drug use focuses on control, forced change, and ensuring, as we have seen, that the experience of drug use is no longer pleasurable. Or, even, that it is punitive...Volkow’s comment about making drug use environments less pleasurable is a bit of an understatement. Researchers and policy-makers have developed everything from fiendishly ingenious ways of making drugs themselves painful, unpleasant, and more dangerous; to ways to render the consumption environment not only not pleasurable but dangerous, traumatizing, and unnecessarily lethal; to creating so-called treatment systems that consistently punish, humiliate, and oppress people seeking help, and indeed are, yes, dangerous as a result. And then, the brain disorder concept of addiction pushes drug users from a coercive criminal justice system to a coercive and controlling medical system on the very inadequate basis of a few studies of functional MRIs relating addiction to patterns of activity in the brain.” OO 276
Again I have no definitive understanding as to what point Carlyn is making here. I believe her point is that the funding agency is putting an emphasis on addiction instead of drug research more generally. I believe her issue is that NIDA is holding a negative view of illicit drug addiction as NIDA actually views drug use as problematic. Carolyn finds issue with NIDA’s premise because her prerogative to defend drug abuse.
It is hard to decipher the ideological background that informs harm-reduction and like everything else it has contradictions and detractors within. Based on my research I am presuming harm-reductionists rely on the BDM to justify their platform but there are circumstances in which they reject it such as labeling drug abusers as “diseased” or accept it when wanting addition viewed as a medical condition instead of a behavioral/criminal issue.
Backpedal
I wrote the previous section against the BDM before I discovered Addiction as a brain disease revised: why it still matters, and the need for consilience, Neuropsychopharmacology 46. This is an apologist piece which admits the criticisms against the BDM are valid yet still promotes it.
For whatever reason they clearly want addiction to be labeled as a disease. The article contains interesting facts about what happens to alcoholics brains, divides addiction from substance use disorder, and defines compulsion.
Above all the article admits its ideological position on life itself:
“Is the brain really a defensible focal point for research and treatment? The answer is “yes”. As powerfully articulated by Francis Crick. “You, your joys and your sorrows, your memories and your ambitions, your sense of personal identity and free will, are in fact no more than the behavior of a vast assembly of nerve cells and their associated molecules”.
“key among those [against the BDM] are claims that spontaneous remission rates are high; that a specific brain pathology is lacking; and that people suffering from addiction , rather than behaving “compulsively”, in fact show a preserved ability to make informed and advantageous choices.”
Critics further state that a “genetic predisposition is not a recipe for compulsion”, but no neuroscientist or geneticist would claim that genetic risk is “a recipe for compulsion”. Genetic risk is probabilistic, not deterministic.”
“but if the criticism is one of emphasis rather than on principle- i.e. too much brain, too little social and environmental factors-then neuroscientists need to acknowledge that they are in part guilty as charged”..”it is not the only lens, and it does not have supremacy over other scientific approaches.”
They admit they offer no solutions neither do they have a plan to anytime soon despite all their funding and research: “the main objective of imaging in addiction research is not to diagnose addiction, but rather to improve our understanding of mechanisms that underlie it. The hope is that mechanistic insights will help bring forward new treatments, by identifying candidate targets for them, by pointing to treatment-responsive biomarkers, or both.”
By now there has been so much push back they have no choice but to defend free-will:
“evidence for a capacity for choosing advantageously is preserved in addiction provides a valid argument against a narrow concept of “compulsivity” as rigid, immutable behavior that applies to all patients.”
But the research isn’t fully wasted:
In her view [Dr. Angell], Big Pharma is a parasitic industry that feeds off publicly funded research. If you look at where the original research comes from on which new drugs are based, it tends to be from the NIH, from the academic medical centers, and from foreign academic medical centers. Studies of this, looking at seminal research on which drug patents are based, have found that about 15 percent of the basic research papers, reporting the basic research, came from industry. That’s just 15 percent” After a drug is developed through public funded research, Big Pharma sells the drug back to the public at extortionate prices, making it consistently among the ten most profitable industries. The US is the only advanced economy that allows companies to charge what the market will bear.” AF 107
Jeff Singer at CATO defends doctors against claims of overprescribing.
(native .008) Fentanyl in Native Communities: Native Perspectives on Addressing the Growing Crisis, indianz, 12/5/2023
Factors outside BDM
“A truism in addiction medicine is that the later a person starts drinking alcohol, smoking, or using drugs. The lower the risk they will become addicted.” AF 167
“the greater the number of adverse childhood events a person experiences, the greater the likelihood that person will suffer from mental health disorders and substance use disorders.” AF 22
“adolescents who use alcohol or cannabis in large amounts to cope with the pain of life are often unable to develop healthier coping strategies” AF 22
Low socioeconomic status, poor parental support, social isolation, and drug availability all affect rates of drug use. AF 23
“Studies show that socially dominant animals have more dopamine receptors in their brain and are less likely to self-administer drugs such as cocaine or alcohol.” AF 23
“Even smokers are at increased risk of abusing opioids, presumably because their brains are already in the business of depending on drugs” AF 25
“nicotine exposure may prime the brain to be more susceptible to other drugs,” AF 168
I referenced how caffeine, nicotine, and alcohol are gateway drugs.
(JASON CHRISTOFF ~“Mind Control Deprogramming From Global Lies & Egyptian Occultism”[Age Of Truth TV], Age Of Truth TV, 4/29/2024)

The study suggested that whether or not adolescents began using nicotine, alcohol, or cannabis was strongly determined by social and familial factors. But as these adolescents grew into adults. Their social environment became less important and genetic factors became stronger determinants of whether they would abuse substances.” AF 21
“someone with ADHD is eight times more likely to have a drug addiction than someone without ADHD.” AF 157
Dr. Ramin gleans over the fact that they are labeled as diseased and prescribed Adderall as if that has no influence on future data gathering.
“kids with ADHD are more likely to have oppositional defiant disorder, conduct disorder, anxiety, depression, and learning disorders, and they are more likely to go on to have substance use disorders.” AF 69
If ADHD is valid, it is grossly over-diagnosed which in my opinion negates studies founded on the diagnosis.
The Goal is not Abstinence
I assert harm-reduction is a means to surveil and coral the most vulnerable. The term Medically Assisted Treatment (MAT) carries a connotation that the goal is treatment and one would assume that treatment amounts to cessation of drug use or at least of dependency.
Injecting with nurse approved technique in a safe place surrounded by caring people and then returning to your stable, affordable apartment- I can’t see how that doesn’t represent recovery…” OO 245
“The dichotomy isn’t between addiction and abstinence. It’s between chaos and stability.”
“The body of evidence we have now about people who use opioids. or most other common illicit drugs simply doesn’t support the assumption that abstinence is either necessary or even -and this a particularity hard pill to swallow, so to speak, for those committed to abstinence -the best choice for all people who use drugs. OO 107
“When people say, ‘Dr. Shyken, aren’t you just substituting one drug for another?’ I say, ’Yes, what’s your point?’ It’s saving lives.” FI 275
“Some measures of success of a treatment are more relevant than others. Buprenophrine and methadone, for example, really do shine at preventing overdose (among those who are able to stick with them, a caveat rarely mentioned out loud). Proponents of abstinence-based treatments tend to tout their success at getting patients off drugs, but rarely mention the extremely high relapse rates or deaths among people who don not respond well to detox or abstinence-based counseling. Where heroin is successful as a prescribed treatment is in restoring a patients quality of life, along with their relationships and communities. The adherence or retention rate- the number of people sticking with treatment for months or years- is also very high (although this is often portrayed as a bad thing, it is actually considered a good thing for most interventions that improve overall health). Overdose deaths in this highly at-risk population decline to zero. Multiple health measures such as treatment for diabetes, viral hepatitis, or HIV improve.. People whose problem was they were drug seeking do extremely well, it turns our, when they find the drug they are seeking.” OO 310
I don’t like to admit this but honesty requires it: I accept that MAT, which includes opioid substitution therapy whether full or partial agonist, is useful in recovery from fentanyl, if not mandatory. Naltrexone is a serious tool which requires a dedication to suffer and sacrifice for abstinence. Naltrexone may not be as pleasant as staying on substitution opioids but it skips the middle man for those who are serious enough to fight for sobriety. I would say naltrexone is a tool for the warriors and Suboxone is the tool for the masses. Both have a valid place in the toolkit.
“75 percent of the patients who had received buprenorphine were still in treatment, but all patients taking the placebo had dropped our of treatment, despite the groups and the counseling” AF 93
Modern Harm Reduction advocates not only disagree but demonize my position as barbaric and ignorant. I do agree that MAT is valid and moral because withdrawal is a living hell which Suboxone/buprenorphine can alleviate but with limited resources we have to set limits. It is not a realistic expectation that anyone can be made free of “pain”. Below are guidelines for those with genuine pain, certainly their needs are more valid than of drug abusers as many abusers initially made a conscious decision to illegally use drugs for recreation.
“Three conditions should be met before such long term therapy is embarked upon: alternatives must fail; the pain must be causing a real impact on the patients quality of life; and the benefits of using chronic opioids must outweigh the risks. Once stared, treatment should be regularly reassessed. Doses should be kept to a minimum and the goals of patients and their providers should be realistic: a reduction in pain, not a life completely free of pain.” AF 114, Rosenquist, Management of Chronic Non Cancer Pain
Sadly pain patients must live within the same paradigm of the recreational addict. As I addressed earlier Carlyn conflates the two.
I am careful not to confuse Fentanyl addiction with other addictions because it is so extreme. In many ways it’s an exception. This exception does not automatically validate the BDM just because the user can’t quit without support. We should not allow BDM scientists to use the exception (fentanyl) as justification for all their other claims. Because Fentanyl is more addicting does not mean we don’t have centuries of insight into addiction.
When they promote “destigmatizaion” their press release’s state it is to destigmatize treatment and therapy. Others, like Carlyn, mean to destigmatize drug users and illicit drug use itself. In practice it looks more like defense and approval and even “pride”. Worse still is their taking offense to those who view drug abuse as wrong. This amounts to me being wrong from condemning drug use and criticizing addicts.
So we are not supposed to stigmatize users. Their feelings matter! We cannot hold them accountable because they are “addicted” card-carrying “victims” who don’t deserve to live under the fear of Justice because that wouldn't aid in their delicate “recovery”. Soon employers will not be allowed to “discriminate” against addicts despite the fact that virtually all sell drugs, steal, or prostitute to fund their addiction. Perhaps drug abusers will next be included in the quota system as a protected class.
Sheetz accused of racially discriminating with worker background checks, by Lizzy McLellan Ravitch, Published April 22, 2024,
Sheetz's policy of screening applicants' criminal history disproportionately affects candidates who are Black, American Indian, and multiracial, the U.S. Equal Employment Opportunity Commission said.
I don’t believe our State is an arbiter of morality or justice but I expect the worst offenders to be “managed” by the state so that they do not endanger the public. Harm-reductionists defend the offenders with no regard for the damage they do. I do not believe in excessive penalties for victimless criminals but I do not entirely absolve their wrong doing either.
“The fifth precept prohibits intoxication through alcohol, drugs, or other means. Early Buddhist Texts nearly always condemn alcohol, and so do Chinese Buddhist post-canonical texts. Smoking is sometimes also included here.” -This article is about the five precepts in Buddhism, Wikipedia
Not only are alcohol, nicotine, and caffeine gateway drugs they are also slow killers. In our society we idolize legal drug dealers in large part because we worship profits. I view caffeine and sugar profiteering as another form of drug dealing. By now I don’t understand why there is not more demand for low-carb, minimally processed, organic foods. Sam Quinones also points to this attribute of our society, he terms the condition of our consumables “drugification”. As well as pandering to a caffeine addiction corporations market sugar (corn syrup) and fat (hydrogenated oil or low quality omega-6 vegetable oil). Perhaps commerce should be measured against a standard of morality or health.
(how overdose .420)
If dealing poison requires a victim look no further than alcohol or tobacco. I may argue clean measured fentanyl is safer than toxins disguised as food. As for the argument that a free market would accompany a cleaner supply, I agree and shared my views in pt 1. But there is no such thing as “free markets”.
Is tobacco addiction wrong? Perhaps addictions are wrong but are dependencies wrong? Tobacco may be considered a dependency instead of an addiction simply because the consequences are farther removed.
“Tobacco is a legal drug, and although it kills one in two long-term users, its use is not linked with the crime or overdoses associated with other drugs. These facts are accidents of neurochemistry and consequences of tobacco's legal and easy availability. In fact, nicotine is nearly as addictive as both heron and cocaine.” AF 20
Ardis challenges whether restricting cigarettes is for public health instead of to weaken us for the next generation of germ warfare. I mentioned his hypothesis on Nicotine, take it upon yourself…
I previously made the comparison between vaping and commercial weed in a paper; I literally titled the paper; Commercial Weed is Dollar General selling E Cigarettes.
“The news about the tobacco epidemic is rather different. For North America, tobacco is a very good news story.” [it has decreased]… the tobacco industry has tried to circumvent anti smoking laws by introducing vaping devices marketed as healthier alternatives to tobacco consumption. Vaping devices are sold with very little regulation and contain carcinogens and additives with unknown long-term health impacts. The e-cigarette industry is booming and is even working with the cannabis industry to create synergies that may very well fuel the addictions of the next generation.” AF 180
“No substance had every become so popular so quickly among American teens [vaping]” AF 181
I would like to add that vaping is claimed to be much healthier than cigarettes. I believe this and recommend people move onto the vapes. Be aware that glycerin is plant based and glycol is from petroleum.
The FDA allows propylene glycol to be used in foods, but there are some health concerns when inhaled
Propylene glycol is a food additive used in many foods and medicine. It can also be found in artificial snow, fog machines, and theatrical productions. Propylene glycol is safe for consumption but it can be harmful when inhaled. The FDA allows propylene glycol to be used in foods, but there are some health concerns when inhaled.
Inhalation of high levels of propylene glycol may cause side effects such as nausea and headaches. If you have been exposed to large amounts of propylene glycol through inhalation or skin absorption please contact your doctor immediately so that they can assess your symptoms and make recommendations on treatment options if needed!
My advice falls on deaf ears of course; I have been preaching for over a decade since fire-safe cigarettes debuted that they contain cancer causing plastic rings and that smokers should be using a bubbler to cool and filter the smoke and not smoking paper.
Dependence
“Not all use of addictive substances or behavior results in addiction. However, a non-addict may choose to engage in a behavior or ingest a substance because of the pleasure the non-addict receives. A non-addict can become an addict through frequency, when an addictive behavior becomes a compulsive action. The change from non-addict to addict occurs largely from the effects of prolonged substance use and the result of behavior activities on brain functioning.” Addiction Psychology Wikipedia
There are countless variations in the likeliness of “addiction” onset but in the end we are dealing with substances that are objectively addictive. But some even argue this fact.
It’s not clear what proportion of the people usually described as addicted are actually physically dependent (due to drugs being used for treatment of long-term severe pain) without exhibiting the behavioral issues that define psychological addiction” OO60
Later I will expose Volkow arguing that opiate use is not “addictive” when she again blurs the definitions between dependence and addiction.
Some believe that "drug dependence" equals "addiction." Others believe that the two terms do not interchangeable. According to the DSM, the clinical criteria for "drug dependence" (or what we refer to as addiction), include compulsive drug use despite harmful consequences, inability to stop using a drug, failure to meet work, social, or family obligations, and sometimes (depending on the drug), tolerance and withdrawal.” Addiction Psychology Wikipedia
That should clear it up!
“perhaps psychological compulsion to use a drug- even when that has profoundly negative effects on our lives- Is really just a social construct, determined by a combination of physical dependence and reduced access. Or, perhaps, a pain patient who loses access to the drug and chooses to replace it in the illicit market or tries desperately to restore access is in fact addicted- was, perhaps, addicted all along… Is that choice what determines whether my physical dependence is an addiction? OO 234, 235
It’s not clear what proportion of the people usually described as addicted are actually physically dependent (due to drugs being used for treatment of long-term severe pain) without exhibiting the behavioral issues that define psychological addiction” OO60
“Much of what is written about opioids., including rather a lot of the medical literature conflates the terms “dependency” and “addiction.” OO60
While many manipulate definitions of “addiction” and “dependence” here it is honestly attempted;
“surely the numbers worldwide depend on conditions of drug availability, social disapproval, and other environmental factors...While it is obviously true that simply trying drugs is not a sufficient condition for becoming addicted to them, I would argue that this is not equally true for humans and for laboratory animals… Most of all, I would not generalize it to humans. Humans are informed about health risks that are not understood by laboratory animals, and it is anticipated rather than immediate consequences that are arguably the strongest deterrent to human addiction, particularly in the case of tobacco smoking. No such communicated deterrent exists for laboratory animals, and in my experience laboratory animals that start taking intravenous cocaine, amphetamine, or heroin never stop taking them voluntarily except when they collapse from exhaustion or convulsions
Wise does not accept ‘dependent’ as a synonym for ‘addicted.’ That said, where along the continuum between volitional and compulsive drug seeking— between initial positive reinforcement and progressively developing positive þ negative reinforcement—is it most appropriate to draw a line and consider an individual or a laboratory animal ‘addicted’?” The Development and Maintenance of Drug Addiction,Roy A Wise*,1 and George F Koob, Neuropsychopharmacology (2014) 39
I don’t want to sell you a conclusion because I don’t have one. These are words, or better referred to as terms and their ambiguity is intentional for rhetorical manipulations. I presented you with different perspectives on the terms and how they are used to reach specific ends, beyond that…
“Some individuals who use opioids go on to develop an OUD. A clinical diagnosis of an OUD is based on the presence of symptoms within a 12-month period on a repeated or recurring basis as outlined in the Diagnostic and Statistical Manual of Mental Disorders (DSM-5).
I admit I have a manageable addiction to kratom but not a dependency. The following criteria claims I don’t have an OUD. “symptoms that qualify them as having OUD (for example, continued intense cravings, continuing to use substances despite negative consequences, persistent desire but inability to stop substance of misuse, etc). An Overview of Medication-Assisted Treatment for Opioid Use Disorders for Criminal Justice-Involved Individuals, Jessica Reichert, Lily Gleicher and Elizabeth Salisbury-Afshar|2017-07-18|(Illinois)
Double minded fakes say what you want to hear
“While Nora Volkow recognized that addiction is a disease of the brain, she pointed out that genes and brain chemicals are not the only agents involved in producing addiction: “Predisposition is not predetermination,” she told a congressional subcommittee in 2005. “Environmental and other biological factors, including family, culture and community, are of great importance to the development of addiction and are essential to it’s prevention.” AF 21
“Studies have proven that genetic variations and differences in our neurobiology can alter an individual's vulnerability to developing an addiction. What causes an individual to be more prone to addiction is their genetic makeup.” Addiction Psychology, Genetic Wikipedia
The likelihood of forming an addiction because of biological or genetic factors is not a cause. This is similar to saying overdose deaths occurred because of a lack of Narcan. Wrong, overdose occurred because of drug abuse. The cause of addiction is not because you were born American Indian or bullied in school. Proof of contributing factors does not prove the BDM explains addiction. You are not addicted to a drug before the first use. If a public expert did care about prevention they would explain that caffeine and nicotine are proven primers for addiction, instead we find coffee product placement on the Disney channel and caffeine in school vending machines.
Dr. James Davies exposes the fraud underlying the DSM manual
Diversion
(panel .633) Panel discussion: Safe supply for adolescents, Addictions and Concurrent Disorders Research Group , 6/4/2024
c060232
[Alfgeir Kristjansson, Icelandic researcher] spelled out the best way to end the epidemic of addiction: preventing or delaying the recruitment of new users. This is the heart of primary prevention, the cheapest and most long-lasting type of intervention in medicine and public health” AF169
The best MAT opioid (Suboxone/buprenorphrine) does not satisfy cravings for fentanyl. Buprenophrine displaces Fentanyl from the receptors. A fentanyl user does not enjoy using buprenophrine and it may cause precipitated withdrawal. They don’t want it unless they are desperate or genuinely trying to quit so very often they divert it, they sell it. The “safe-supply” that users do want is legal heroin and fentanyl. Safe supply is direct substitution and fully enables the addict. Safe supply and harm-reduction are not treatment and when you get specific they don’t claim to be.
At risk of beating a dead horse;
watch Racheal squirm and avoid admitting that safe-supply is not the same as MAT because giving meth and fentanyl to children is still controversial
Panel discussion: Safe supply for adolescents, Addictions and Concurrent Disorders Research Group , 6/4/2024 (.595)
“We don’t encourage drug use, but our goal is to eliminate unnecessary harm.” FI 271
“studies of methadone, buprenorphine, and injectable opioids similarly show that people on treatment commit fewer crimes.” AF 127
“to provide a safe supply of opioids such as morphine and hydromorphone to those who use drugs.. to provide a safe supply of opioids to people at safe consumption sites for use on site, instead of them having to bring in contaminated fentanyl.” AF132
switching to another opioid only puts the problem off for another day” AF 77
The public will come to understand, too late, the goal of harm-reduction is not abstinence. I contend the goal of harm-reduction is instead policies toward safe-supply. Recovery is redefined.
I would argue not only does enabling extreme opioid use postpone the negative consequences of drug use but also strengthens addiction. Time may heal all wounds but it also strengthens addictions.
I left in my previous claim, which was incorrect, as an example of how easily we can believe our assumptions. There has been a lot of research in this particular area navigating the vast sea of medical literature of this field I stumbled upon it. Actually the conclusions also refute the disease model.
“Thus, each year a constant proportion of those still addicted remitted, independent of the number of years since the onset of dependence… Although varied [according to the specific substance], the remission results were orderly. An exponential growth curve closely approximated the cumulative frequency of remitting for different drugs and different ethnic/racial groups. Thus, each year a constant proportion of those still addicted remitted, independent of the number of years since the onset of dependence. People Control Their Addictions, Stanton Peele
Since drugs change the brain, these results suggest that the changes do not prevent quitting, and the slope of Figure 1 implies that drug induced neural changes do not even decrease the likelihood of quitting drugs once dependence is in place...
Figure 1 shows that the likelihood of remission was constant over time since the onset of dependence. Although this is a surprising result, it is not without precedent. In a longitudinal study of heroin addicts, Vaillant reports that the likelihood of going off drugs neither increased nor decreased over time” Addiction and Choice: Theory and New Data Gene M. Heyman (this paper will be cited ad naseum later)
*
“Calls for safe supply blended with calls to decriminalize drug possession.” AF 132
Are these not separate issues each subject to individual criticism?
Only when we view promotion of drug abuse as cultural subversion can we understand why harm-reductionists universally accept all the tenets. My position is that recreational drug use is objectively wrong. I recreationally use kratom. I know it is a safer recreational drug as well as a great tool for those with legitimate pain needs but I will not deny my own hypocrisy. I have used kratom and coffee as a tool to quit other drugs. I am now proudly 3 years sober from both alcohol and marijuana. I should not use kratom recreationaly but for me presently the benefits outweigh the costs. I am not arguing that my actions are right, true, and Good but instead I admit my shortcomings while I continue to use. This is the difference between my recreational drug use and the ideology promoted by harm-reductionists. They wish to destigmatize and accept (non pain-management) opioid addiction if not defend, promote, and celebrate it.
“Isn’t opening the spigot on the opioid supply exactly what got us into this problem in the first place? The parallel does not hold up, however, as safe supply advocates are looking to prevent death in those already using high-risk opioids., rather than introducing new people to opioid use. The details of any programs will need to be carefully planned, and the programs will need to be monitored and then regularly reevaluated” AF 133
Legalization of drugs automatically excludes “planning” or “monitoring” or “reevaluating”. MAT Suboxone is not desirable for fentanyl users so where is it diverted to? Is it finding its way to people who are trying to quit outside of the system? Unlikely, because most can attain the same MAT services. This may be debatable as providers are scarce, as is healthcare, and centers may even refuse to allow back those who previously abused the programs. When Suboxone is diverted to individuals using it as a tool to better themselves it begs the question “What is the seller doing with the money?” I presume most are buying Fentanyl. My friend pushed back; “some people attain abstinence but keep their Suboxone script just to help others.” I’d like to believe this but those who quit Suboxone/Buprenorphine likely tapered down over time so I presume have smaller and less dosages, their may also be some type of testing to continue their prescriptions; this also assumes the minority who managed to attain complete sobriety and keep a suboxone prescription (which is dishonest) are not merely selling drugs to anybody who will pay but instead only selling to those trying to quit and not to new users. Diversion can be made a moot point as extended release injectable buprenorphrine is gaining popularity which only requires long intervals between administration without drugs leaving the clinic. This could be good to prevent diversion (new users using a gateway drug) but bad for those outside the system who need the MAT to combat fentanyl addiction on their own, those who intentionally avoid the medical industrial complex.
There are many parallels to marijuana. Medical marijuana has been the thin end of the wedge. The goal of the movement was never to use marijuana for glaucoma or seizures but was just a great excuse to promote and idolize of a drug fueled lifestyle (Not to discount some individuals compassionate medical intentions). In Michigan, what came of it was over-prescribing marijuana for anyone with a pain history with the boundaries being extended toward (subjective) anxiety. I am not wholly against the outcomes of the medical weed here in Michigan, a lot of small-timers made money, quality went up, and not unimportantly legitimate pain patients had another tool at their disposal. But the corollary is significant. I allege safe-supply is not for problematic opioid users obtaining tools for self betterment but instead the medical justification is propaganda which papers over the agenda to further destroy culture and values.
c060232
(a year in .592 3)
I myself, while doing this research, have considered trying Suboxone, curious because it is said to have a low potential for abuse. I bet it would mess me up pretty good though! If I thought of experimenting with diverted MAT drugs you can bet some confused 15 year-old has as well. This risk of diversion of buprenophrine or Suboxone may not be as bad as dangerous as full-agonists and safe-supply but buprenorphine still carries real risks. Those seeking “recovery” would only need substitution drugs temporarily to taper down on their way to abstinence otherwise they would need their own consistent and reliable supply for years. Yes, some people can use the black market to quit but these stories are exceptions.
I spoke with a healthcare worker from a local addiction center and he informed me, with certainty, that the MAT drugs they provide can be easily abused by beginners. Buprenorphine is very addicting by way of negative reinforcement. Ginny also confirmed the gateway drug hypothesis during our phone call.
They are strategic in how they defend their program on paper but how do do these centers and pop-up tents operate in practice?
[Regarding his meeting with Scott MacDonald] “I worried people would abandon their stable life on methadone because of the temptation of free and safe injectable heroin. He put my mind at rest, reminding me that injectables are the most intensive step on the the treatment ladder. This means two things. First, only the patients who have continued to relapse while on every other type of treatment will need injectables. Second, the time and inconvenience of having to make multiple visits to a clinic every day means that many people will choose to simplify their treatment over time. [in countries like Switzerland] where many people drop out of injectable treatment and return to the relatively simple treatment of methadone over the long term.” AF 102
I would like to add these aren’t just some examples. After hundreds of hours of research I present all the justifications I’ve come across.
Their first excuse: “only the patients who have continued to relapse while on every other type of treatment” relies on and insinuates that only those who have failed other treatments will be allowed safe-supply. But is this borne out in practice or will they grant access to anyone?
It also assumes and requires government or charities to fund and promote safe-supply drugs to users unconditionally and forever (A later example I provide pressures the Mexican government to accept the program). As stated; the only criteria is users who fail at recovery will have access to safe-supply. What is the other criteria to acquire these drugs, who decides it, is it subjective? Maybe I want free heroin, does this create an incentive for me to worsen my addiction or drop out of programs?
“Joe would do anything to be able to get back the self he had when he had access to “real” opioids. Anything except risking fentanyl-contaminated street opioids. But to be prescribed real opioids, you need to have a worse case of opioid use disorder than he is considered to have. How would you demonstrate that you are sick enough with addiction to qualify for an opioid substitution program? Well, you’d be someone who persistently uses street opioids.” OO 240
It also assumes drug manufactures can even provide these controlled substances. And without a concern for international treaties and local drug laws, as this is allowed to progress it proves the globalist agenda finds little resistance from local government. What if these drugs have no prescription counter part as many are Novel Psychoactive Substances (NPS). Most recently we have medatomidine (zloxine, nitozine) which doesn’t trigger test strips or respond to Narcan. Harm-Reductionists suggest that if for any reason a user doesn’t want to quit the state should subsidize drugs for addicts. There may now be too many fentanyl analogs to list, cafentanyl is much stronger than fentanyl, is the expectation that every variety will be provided accessible? And what of the laws that regulate their distribution, are drug companies automatically dismissed from oversight and what about the chain of custody which accompanies controlled substances? Why even have licenses to prescribe or administer these drugs if regulations are drastically lessened? And if we are instead looking to the black market for these drugs this raises more questions. Who are these volunteers in pop-up tents and how can we trust them to not divert them? Will purple-haired 23 year old unicorns, likely drug addicted themselves, be given authority and discretion to distribute illicit drugs?
Their next excuse is based on inconvenience “Second, the time and inconvenience”. We are expected to believe that because safe-supply may be inconvenient that users would prefer to simplify their treatment over time. As if maintaining a Suboxone addiction is such a cake walk, when the clinics closed, or the pharmacy is out, or you lost your script for any reason, or you moved, or lost your doctor. The pop up free drug tent is open! Perhaps they don’t provide Suboxone but only safe-supply, maybe it’s just a safe injection site, perhaps you would prefer to not face the temptation to chose. This is the ground shattering excuse by the same groups fighting to remove barriers-to-access and destigmatize and legalize drug abuse. Is it also inconvenient to stop at a vending machine?
[Mark Tyndall, head of the BC Centre for Disease Control] “I had an idea to put up vending machines that dispense opioids.”… “to give away opioids. in order to prevent users from purchasing heroin and fentanyl. AF 132
“The idea was to have highly secure steel units dispense doses of hydromorphone to users registered to the system. The machines would use biometrics to verify the identity of registered users and then dispense their dose.” AF132
Apparently they have no concern that vending machines will not prevent diversion and are unlikely to be immune to hacking or theft.
“[Scott said] don’t wait until fentanyl comes to your community to start a program like this.” AF 103
Let me rephrase this: Don’t wait to give out state sanctioned full-agonist opioids to the public instead provide anyone who wants to get high with clean drugs and the tools to use them now! This is expert logic when we prioritize the needs of drug addicts over Prevention. Perhaps the statement should read don’t wait until the public is addicted, addict them now so the state can manage it. I struggled to understand what he meant by this because there are supposed to be requirements and vetting for the program; he must be referring to existing heroin or pain-pill users. Either way I made my position clear against safe supply while I grant some legitimacy to MAT (Suboxone/ buprenophrine).
Dr. Turnbull co-founded OICH and their equally controversial managed alcohol program (MAP). [which] reduces binge drinking and prevents life-threatening alcohol withdrawal by providing small amounts of wine every hour to people with severe alcohol use disorder...Turnbull began to wonder if the initially counterproductive practice that works so well with MAP- simply giving a substance-seeking, substance-dependent person a quality-controlled version of the very substance they are seeking – could work for opioid-addicted patients as well.” OO 243
Focus gets results
(thisisaveryweird .195)
Are studies based on addicts who receive more focus in a more controlled setting maybe even with more wrap around services going to achieve better results despite the specific variable being tested for. Such as those taking MAT or safe-supply VS those not receiving any of that attention. Are the studied participants in-patient, are they given housing vouchers during the the test, are they given access to other medical treatment, maybe even money which can aid their health? The other issue is how do you measure the baseline, the control group who is not involved in any part of testing and therefore can’t be quantified or evaluated.
Test strips
One tenet of harm-reduction I can agree with are testing strips (drug checking). In a cost-benefit analysis they have overarching benefits.
In principle the state should never endorse or enable any illegal behavior as this undermines its own authority. Therefore I understand the logic behind banning drug checking (test strips). Their purpose, above all, is to enable illegal drug use. Navigating the black market may carry penalties but does the punishment fit the crime? What if a test strip is only to detect contaminates in a schedule 4 drug? Should it be treated equal to a meth pipe? I’m sure test strips are used in a way to prevent exposure to fentanyl. This sword cuts both ways. I advocate for minimal penalties, if any, for drug checking paraphernalia.
This is an example of accepting some tenets of the far-left agenda. Compromise and our ability to articulate very specific situational criticisms is our only chance at holding back this tidal wave. Modern politics only exasperates the divide. I have news for you if you haven’t figured it out yet: Nora Volkow and the far-left UN agenda are going to win out. Conservative’s murder charges and increased persecutions may gain footing but institutionally, harm-reduction ideology will prevail to the point of guiding policy. The fact that you don’t know anything about this topic, which is arguably the only real epidemic we have ever experienced, is evidence that your knowledge and participation in law or the surveillance economy is not required. When your kids bring home clean needles maybe you will begin your crusade but you wouldn’t know where to start would you? It’s already too late to change the trajectory but at least you can understand it. You ignorance is more than welcome; It’s China’s revenge for the Opium War, It’s the border, It’s the cartels, It’s the liberals; mere sound bytes that feign insight yet contribute nothing.
“a 2017 study carried out at a supervised injection site in Vancouver, BC, found that those who discover fentanyl in their drugs are ten times likelier to lower their dose, which makes them 25 percent less likely to overdose. A 2018 study released by Brown found that among RI users whose drugs tested positive for fentanyl, 45 percent reported using a smaller amount, 42 percent proceeded more slowly during their use, and 39 percent used with someone else present, who could give them Narcan…” FI 247
The ONDCP plan includes worthy harm reduction recommendations, such as making it easier for users to test their drugs for xylazine. The makers of fentanyl test strips have already developed xylazine test strips, but, unfortunately, many states still outlaw drug testing equipment or devices as drug paraphernalia. While many states have recently removed fentanyl test strips from their list of illegal paraphernalia, their lawmakers would need next to remove xylazine test strips from that list. It would be wiser for states to remove all testing equipment and devices from their lists of banned paraphernalia. Even better, as Minnesota recently did, they should repeal their paraphernalia laws altogether.- The White House Addresses Tranq While Lawmakers Fight The Last Battle Against Fentanyl Analogs By Jeffrey A. Singer
“Gladys Berejiklian “Unfortunately we know that pill testing won’t work because it will give people the green light to take substances which in the end could still kill them.” FI 274
paraphernalia
“such zero-tolerance drug paraphernalia laws can lead people who inject drugs to fear carrying syringes and force them to share equipment or dispose of it unsafely”. AF 119 “...but I do understand the counter argument “We can’t afford to create a false sense of security… let’s not rationalize putting tools in place to help [drug users] continue their lifestyle more “safely.” Elinore Mccance-Katz FI 274
Drug checking won’t help if users are seeking fentanyl, it only works as prevention from fentanyl use but many will use contaminated substances anyway even with knowledge of the adulterant as evidenced above (2017 BC study). Therefore benefits do exist but are certainly not absolute.
(Whats new in addiction .922) What's New in Addiction Medicine Vol 65, British Columbia Centre on Substance Use, 5/9/2024
So what if drug abusers find out their drugs are contaminated and use less. The point is they are using fentanyl. I don't care the dose. I doubt fentanyl’s addiction potential is dose dependent. Once beginners are using any dose we have failed at Prevention. Just because they don’t overdose this time, what about next time?
As if using less fentanyl or administering it slower won’t lead to addiction, and (despite occasional use of safe injection sites) addiction won’t accompany risky behavior later. But what grieving parents want to hear is that we launch a campaign bombing Mexico laboratories, or give dealers mandatory minimums instead of accepting the fact that they raised their foolish children to knowingly and voluntarily ingest this. These studies confirm that a statistically significant amount our drug addicted young adults are not accidentally using fentanyl.
Drug checking falls under both Prevention and Harm-Reduction. Harm-Reductionists defend drug use so they tread carefully to ensure they don’t endorse or invest in Prevention. So do flowery endorsements of drug checking (test strips) outshine the anti-drug message of Prevention campaigns; Use responsibly VS don’t use at all.
Narcan falls under the category of harm-reduciton not prevention. They consider Narcan prevention because it prevents overdose. Narcan does not prevent drug use but it does provide a false sense of security. Narcan without additional treatment only prolongs death, even for as little as hours until they score their next dose.
Can we positively pin dealers with murder if the deceased was previously addicted to fentanyl and seeking fentanyl?
“overtime people who use street opioids. have gone from unintentionally overdoing due to unsuspected presence of fentanyl to simply accepting the greater risk, to being dependent on illicit fentanyl and actively seeking it rather than heroin.” OO80
AA
Carolyn bashes the AA/NA model instead of including it as one the few existing organizations which may benefit some users especially because of it’s open-door anonymity policy with no barriers to entry. Everyone is welcome with no requirement for admission or participation. Most significantly, there is literally nothing meaningful being done for “prevention”. Listening to drug users complain about how drugs wrecked their lives is probably the best prevention your going find.
“AA is unresponsive to evidence, and focused on shame-inducing interventions that don’t work, or that don’t work well enough for enough people.”
She lies by omission again ignoring the fact that many abstinence-based programs have began accepting opioid substitution therapy. Instead she cuts off the nose to spite the face!
She cites a 2019 study by Sarah Wakeman that found only treatments which used opioid substitution therapy lowered risk of overdoes..”not with counseling, but simply on their own”. This is her “proof” to reject the entire institution of AA/NA? Does she really care about providing people with accessible recovery tools or is she more interested in attacking “conservative” institutions?
Meanwhile Wakeman study again confirms my position (which is explained thoroughly in Pt 1 https://mattcircus.substack.com/p/money-for-fentanyl that wrap-around services are a luxury which is costly and unnecessary.
* author I like who doesn't like AA
this is a very weird .482, .266
JAIL
As we deal with this mass casualty situation with limited resources progressives hate the prison-industrial complex which targets victimless drug criminals as much as I do. With continued access to opioids most will never seek treatment and of those who graduate detox most will relapse; I admit that incarceration is a useful tool, if not the most useful to attain some form of recovery. Progressives can not accept this truth because it would diminish their loudest solution; decriminalization. Harm-reductionists should pivot their efforts and focus on jail reform. Sadly I wouldn't put much faith in any of their solutions as their efforts all conform to one agenda.
Recently locally, 5-23-24 Harbor Country News announced Sobriety court proposed for Berrien County by Julie Swidwa.
“Roscoe told the committee that people who are charged with a second drunken driving offense would become eligible for sobriety court. They would be paced on two years probation, rather than put in jail, and would be granted a conditional driver's license. [Lafond said] “It’s effective, accountable treatment. It’s great for participants, the courts and the community.”.. “This court would help people and their families. If people go to jail, they are unable to go to work and support their family.”
unrelated from the same article: “The average drunk driver has driven drunk 80 times before a first arrest, based on 2011 data... CDC.”
The issue with fentanyl is that it is almost, if not fully impossible to quit without assistance. With weak families and community, and a corrupt society I can’t envision any solution besides forced incarceration. If One can avoid jail for kidnapping, their loved ones would probably be safer fighting withdrawal locked in One’s garage (as long as One introduces Suboxone correctly).
GABOR MATE
Another model of addiction is the self-medication model (or drive-reduction).
In fairness, I am very surprised Carolyn holds my position against Gabor’s claims. She wrote my criticism better than I could have. I am not against holistic tools and techniques such as CBT (but I am skeptical if resurfacing buried traumas is always helpful). In reality yoga and coloring books are not a magic bullet during Fentanyl withdrawal.
“[Gabor Mate] claims “drug use is a misplaced coping mechanism”, and “a forlorn attempt to solve the problem of human pain.” His mantra is “The question is not why the addiction, but why the pain.”...this assumes, despite evidence to the contrary, that all “hard” drug use is a tragic response to trauma… it replaces the addict as monster trope with the addict as patient, or as child..
But while a valuable counter to theories of addiction that focus too much on personal responsibility, Mate’s view tends to promote a paternalistic view of people who use drugs that can prevent drug user organizing, diminish interest in policies that respect user autonomy and informed choice, and be reductive, improbably pinning all addictive behavior on unresolved psychic wounds or , even less credibly, on trauma-inducing damage to brain receptors..
An exclusive focus on early childhood trauma as explaining addiction (or pain) risks overly minimizing the outsized impact of ongoing traumas like poverty, poor-bashing, racism, and homelessness; the impact of prohibition itself, and even the revolving door, poor-quality, paternalistic addiction treatment system; or the way addiction treatment is rarely based in good evidence and even more rarely based in empowerment and rights for people who have been chronically oppressed.
Framing drug use as a misguided response to trauma also ignores the inconvenient fact that the vast majority of those who try opioids, whether medically, recreationally, or for self-medication, never become addicted… pain patients, too, are thought to be infantilized by their suffering, unable to accurately understand or express their own needs.”160-162OO*
One school of thought is for trauma based therapy. Admittedly I did not research this perspective much. I’m sure the topic is well developed but I don’t have much faith in these forms of therapy (coloring books, memory recollection) as they are mild for a powerful addiction; Of course they aid in self- development which never hurts, perhaps they provide enough introspection to find the desire to quit. Overaying their evidence with the BDM, behavioral modifications seem contradictory to an alleged “biological/ genetic predetermined”.
Volkow’s contradiction:
“Unlike tolerance and physical dependence, addiction is not a predictable result of opioid prescribing. even among those with preexisting vulnerabilities.. recent studies have shown that the molecular mechanisms underlying addiction are distinct from those responsible for tolerance and physical dependence, in that they evolve much more slowly, last much longer, and disrupt multiple brain processes.”
“The repeated administration of any opioid almost inevitably results in the development of tolerance and physical dependence.”
In contrast, addiction will occur in only a small percentage of patients exposed to opioids. Addiction develops slowly, usually only after months of exposure, but once addiction develops, it is a separate, often chronic medical illness that will typically not remit simply with opioid discontinuation and will carry a high risk of relapse for years without proper treatment.” Opioid Abuse in Chronic Pain — Misconceptions and Mitigation Strategies, Nora D. Volkow, M.D., and A. Thomas McLellan, Ph.D. March 31, 2016
Here our BDM hero Nora Volkow in 2016 downplays the likeliness of addiction, going as far as to claim “only after months”, then she continues to muddy the waters between dependence and addiction; “but once addiction develops, it is a separate”. After the article I still don’t get her point. A point she labors to make but doesn’t have any practical significance and almost a full decade later still isn’t actionable other than absolving the guilt of drug abusers. According to her addiction occurs “ usually only after months of exposure”. By her logic I can then infer illegal drug use (breaking the law and jeopardizing your family and community) is a conscious decision for months.
from the same article for general education:
“In particular, tolerance to the analgesic and euphoric effects of opioids develops quickly, whereas tolerance to respiratory depression develops more slowly, which explains why increases in dose by the prescriber or patient to maintain analgesia (or reward) can markedly increase the risk of overdose.” Misconceptions 2016
Rephrased; your tolerance increases faster than your respiratory system can adapt to the increases, so increasing dosages exponentially increases risk of death. This is not so with kratom or buprenophrine.
Carolyn not an addict
Carlyn further succumbs to her own delusions; “I still do not have an opioid use disorder, nor do most long-term, daily prescription opioid users- even though now I, like most of them, have a level of physical dependency. If we stop using the drug suddenly we’ll experience withdrawal symptoms… The fact that having such symptoms and trying to regain access to the drug so closely resembles the symptoms of opioid use disorder can be interpreted different ways… Perhaps psychological compulsion, to use a drug- even when that has profoundly negative effects on our lives- is really just a social construct, determined by a combination of physical dependence and reduced access… Is it possible that the behavioral aspects that make up a diagnosable substance use disorder are merely predictable artifacts of a situation where dependent people are deprived of the drug they physically require? That people with addiction to opioids like heroin or illicit fentanyl are really just physically dependent but denied a level of access I have to the drug I need?.. Is it possible that addiction to a drug like heroin, doesn’t really exist?.. [Meg] She distinguishes between self-medication of trauma and pain, and addiction.” OO 234 236
According to Carlyn illicit heroin dependents are not addicts! And if Meg is “self medicating” for “trauma” she is not an addict either.
“I [Carlyn] tell him that they have been a revelation in that they give me control over depression. I confide bashfully that while I am taking them as prescribed and in modest doses for pain, I do choose when to take them more on the basis of enjoyment, especially on quiet evenings when I write.” OO54
“In a way it seems that I’m [Carlyn] insistently trying to establish myself as being “on the edge” of being an addict; gently he pushes back, defining me with equal insistence as a person doing the best she can. According to the biophychosocial approach to addiction, just because something is highly pleasurable, illegal, or dangerous doesn’t mean anyone who uses it will fall prey to addiction (statistics for just about any potentially addictive substance you can think of bear this out). Addiction is far more complex, and results from an individual combination of an experience feeling immediately rewarding, of biological predisposition, of availability of the pleasure substance, of our relationships with other people, and of physical and emotional suffering that may be relieved by the behavior or substance. Skinner speaks generally about addiction, which includes behaviors like compulsive gambling or porn addiction. But there are substances- like opioids- that seem to invite dependency.” OO54
“I don’t tell the family doctor the pain killers make me high- or alter my experience of reality- and he has never asked. In an enlightened age of medical cannabis, it wouldn’t really be an appropriate question. Besides, most people taking opioids. as prescribed to relieve constant pain would quickly develop tolerance and lose any euphoric sensations, making them only early, emergent properties…” Carlyn OO 48
“so what I think I’m craving is the pain relief rather than the opioid itself.” OO 53
I enjoy recreational use of kratom, I am able to maintain my “addiction” to it. Some people get very addicted to kratom and very sick from withdrawal. I set limits for myself. I am able to do this because I did the research and used foresight when I began. I may use it two days in a row which breaks one of my rules but I do so consciously and cautiously. I have more self control over my kratom usage then I do over snacking! But I do like using it for certain occasions and do not wish to quit which I believe constitutes addiction (this is arguable since many define addiction as having bad repercussions) but I am in full control of how often I use. I have used this drug in different ways for 10 years which is certainly long enough for any type of serious addiction to develop. I have quit for long periods of time to test myself. I am not outside of its reach for addiction, at times I feel a desire to use. Many days I chose not to act on my desire but it really wouldn’t matter if I used or not. My history with kratom is evidence against the BDM's claims that my neural circuits are now rewired although I do experience it’s potential for addiction. I chose to deny myself, I doubt my genes or brain chemistry have any role in this. If anything I have a very addicting personality, I once smoked at least 2 packs a day and smoked weed every 20 minutes for years. I can’t choose how good the drug makes me feel or how it effects me but I do choose when and how often to use it. I admit if I was simply chased pleasure with no self-control I may have developed a serious problem by now but if that was the case kratom wouldn’t be my drug of choice either.
My story is not special except that kratom can be mild and correct administration takes effort. A traditional opioid would be much easier to over-use. I make a great case study regarding definitions! I do not have dependence on the drug because I don’t need it physically at all.
Funny story; There was an incident when I was hurt and decided I should use real pain medicine so I reached out to the “informal market” forgetting that I promote kratom. Isn’t it funny how innocent this story is. Needless to say when I realized I had the medicine under my fingertips it was pretty satisfying; risk taking was not necessary! I wasn’t seizing an excuse to use a “real” opioid (although I was questioning myself). I already had the medicine I needed.
I can chose to not use kratom for weeks if I feel like it (such as for 7 weeks while I edit this, but mostly because I decided to quit caffeine awhile because of Jason Christoff ). Usually I don’t use until the weekend which is pretty good evidence that I am in control, if I use midweek it doesn’t concern me but I raise the yellow flag. I decided that I am addicted because I don’t want to quit and I have cravings. Any negative effects are mostly benign but it’s very effective as a substitute for other drugs. Like all drugs it causes mood swings but nothing close to weed! The cessation of mood swings was the first major effect I noticed after I quit pot, an effect most stoners aren’t able to perceive about themselves. When I surround myself with friends who drink and smoke I feel I am a good example. I have found the only people who adopt kratom do so because of real opioid withdrawal or pain. Only because I wanted to quit alcohol and weed was I able to appreciate kratom; it is so mild and administration is so finicky it doesn’t lend itself to recreational use very easily. Most YouTube videos addressing severe kratom withdrawal are likely due to the fact that the users already have a preexisting opioid addiction they are using kratom to assist with, their dosages are crazy; as a precaution I don’t mess with kratom extracts.
“What accounts for apparently simultaneously increasing painkiller and heroin addiction rates in the early part of this century, along with the sharp increase in measured alcohol use disorders? It is certainly not a good sign for current conceptions of addiction and therapy for it, but rather the reverse (Peele, 2015). In Recover! (Peele and Thompson, 2015), I argue for therapy that (a) separates people's identities from their addictions by making clear the latter are changeable, and (b) the use of mind- fullness, derived from Buddhism, that presents cognitive techniques that allow people to detach themselves from the ongoing rush of their experience People control their addictions, Stanton Peele
his remarkable finding about addiction as experienced “in the flesh” won't impact those who espouse chemical remedies for addiction, and who detest self-cure,” People control their addictions.. We issue a call in Recover!: "So, hear this: you are not a passive spectator to your brain's functioning or an unfortunate victim of it. You are the primary generator of how your brain functions—of how you function—both in the here and now, and certainly over the long run."
And this is free will. People control their addictions, Stanton Peele
*
I can’t justify paraphrasing this article any shorter, your here for the fine points:
Addiction and Choice: Theory and New Data, Gene M. Heyman
Addiction’s biological basis has been the focus of much research. The findings have persuaded experts and the public that drug use in addicts is compulsive. But the word “compulsive” identifies patterns of behavior, and all behavior has a biological basis, including voluntary actions. Thus, the question is not whether addiction has a biology, which it must, but whether it is sensible to say that addicts use drugs compulsively. The relevant research shows most of those who meet the American Psychiatric Association’s criteria for addiction quit using illegal drugs by about age 30, that they usually quit without professional help, and that the correlates of quitting include legal concerns, economic pressures, and the desire for respect, particularly from family members. That is, the correlates of quitting are the correlates of choice not compulsion. However, addiction is, by definition, a disorder, and thereby not beneficial in the long run. This is precisely the pattern of choices predicted by quantitative choice principles, such as the matching law, melioration, and hyperbolic discounting. Although the brain disease model of addiction is perceived by many as received knowledge it is not supported by research or logic. In contrast, well established, quantitative choice principles predict both the possibility and the details of addiction.
Addictive drugs change the brain, genetic studies show that alcoholism has a substantial heritability, and addiction is a persistent, destructive pattern of drug use. In scientific journals and popular media outlets, these observations are cited as proof that “addiction is a chronic, relapsing brain disease, involving compulsive drug use”.
Yet, research shows that addiction has the highest remission rate of any psychiatric disorder, that most addicts quit drugs without professional help, and that the correlates of quitting are those that attend most decisions, such as financial and familial concerns.
Thus, in order to explain addiction, we need an account of voluntary behavior that predicts the persistence of activities that from a (long term) are irrational. That is, addiction is not compulsive drug use, but it also is not rational drug use
By year 4 (since the onset of dependence) half of those who were ever addicted to cocaine had stopped using cocaine at clinically significant levels; for marijuana the half-life of dependence was 6 years; and for alcohol, the half-life of dependence was considerably longer, 16 years. As the typical onset age for dependence on an illicit drug is about 20, the results say that most people who become addicted to an illicit drug are “ex-addicts” by age 30. Of course, addicts may switch drugs rather than quit drugs, but other considerations indicate that this does not explain the trends displayed in Figure 1. For example, dependence on any illicit drug decreases markedly as a function of age, which would not be possible if addicts were switching from one drug to another
The correlates of quitting include the absence of additional psychiatric and medical problems, marital status (singles stay addicted longer), economic pressures, fear of judicial sanctions, concern about respect from children and other family members, worries about the many problems that attend regular involvement in illegal activities, more years spent in school, and higher income. Put in more personal terms, addicts often say that they quit drugs because they wanted to be a better parent, make their own parents proud of them, and not further embarrass their families. In short, the correlates of quitting are the practical and moral concerns that affect all major decisions. They are not the correlates of recovery from the diseases addiction is said to be like, such as Alzheimer’s, schizophrenia, diabetes, heart disease, cancer, and so on
This is relevant because a common feature of addictive drugs is that they provide immediate benefits but delayed costs. Thus, it is possible that the drug is the best choice when the frame of reference is restricted to the current values of the immediately available options but the worst choice when the frame of reference expands to include future costs and other people’s
needs. According to this account, persistent drug use reflects the workings of a local optimum, whereas controlled drug use or abstinence reflects the workings of a global optimum [short term vs. long term benefits]”
As self-administered drug doses greatly exceed the circulating levels of their natural analogs, persistent heavy drug use leads to structural and functional changes in the nervous system. It is widely – if not universally – assumed that these neural adaptations play a causal role in addiction. In support of this interpretation brain imaging studies often reveal differences between the brains of addicts and comparison groups. However, these studies are cross-sectional and the results are correlations. There are no published studies that establish a causal link between drug-induced neural adaptations and compulsive drug use or even a correlation between drug-induced neural changes and an increase in preference for an addictive drug.
most addicts quit. Thus, drug-induced neural plasticity does not prevent quitting.
Since drugs change the brain, these results suggest that the changes do not prevent quitting, and the slope of Figure 1 implies that drug induced neural changes do not even decrease the likelihood of quitting drugs once dependence is in place
Figure 1 shows that the likelihood of remission was constant over time since the onset of dependence. Although this is a surprising result, it is not without precedent. In a longitudinal study of heroin addicts, reports that the likelihood of going off drugs neither increased nor decreased over time
Twin and adoption studies have repeatedly demonstrated a genetic predisposition for alcoholism, and the limited amount of research on the genetics of illicit drug use suggests the same for drugs such as heroin, cocaine, and marijuana. However, all behavior has a genetic basis, including voluntary acts. The brain is the organ of voluntary action, and brain structure and development follow the blueprint set by DNA. Thus, there is no necessary connection between heritability and compulsion. In support of this point, monozygotic twins are much more likely to share similar religious and political beliefs than are dizygotic twins, even when they are separated before the age of 1 year old. That is, learned, voluntary religious and political beliefs have substantial heritabilities just as do many involuntary human characteristics. The relevance to addiction is that a genetic predisposition is not a recipe for compulsion, just as brain adaptations are not a recipe for compulsion.
[My note: this argument was hard for me to grasp. Pay attention to the authors distinction between voluntary and compulsion.]
addiction involves an initial “honey moon” period, followed by alternating periods of remission and relapse, and then an eventual return to a more sober life. Most addicts quit using drugs at clinically significant levels, they typically quit without professional help, and in the case of illicit drugs, they typically quit before the age of 30. The correlates of quitting include many of the factors that influence voluntary acts, but not, according to Figure 1, drug exposure once drug use meets the criteria for dependence. Thus, we can say that addiction is ambivalent drug use, which eventually involves more costs than benefits (otherwise why quit?). Behavioral choice principles predict ambivalent preferences, semi-stable suboptimal behavior patterns, and the capacity to shift from one option to another. In contrast, the brain disease account of addiction fails to predict the high quit rates; it fails to predict the correlates of quitting; it fails to predict the temporal pattern of quitting; and it is tied to unsupportable assumptions, such as the claims that neural adaptations, heritability, and irrationality are prima facie evidence of disease. To be sure “compulsion” and “choice” can be seen as points on a continuum, but Figure 1 and research on quitting make it clear that addiction is not a borderline case
These same choice models also predict that individuals caught in a destructive pattern of behavior retain the capacity to improve their lot and that they will do so as a function of changes in their options and/or how they frame their choices. This viewpoint fits the facts of addiction and provides a practical guide to measures that will actually help addicts change for the better.
Consent
I acknowledge the corruption of our institutions but I will not discount the benefits of our political system. If I had to summarize what I know about our legal system in one word it might be consent. As if we can remove our consent! As if there is any choice but to participate in society! As if reading the terms of service of our computers operating system or mortgage or “voluntarily” perjuring ourselves paying income tax accompanies any legitimacy. Our government is run by extortion, force, and coercion. Progressives don’t realize that abstract rights are a radical revolutionary idea, they already won their ideological war. Their leaders, not true to any ideology other than power, wish to destroy any semblance of local government for globalism or rule of the international elite. The left is better organized and better educated in science as well as legal subversion. Today schools primarily teach ideology and activism. The managerial class will troubleshoot the technological-surveillance grid and the masses will feed and power it. Since when does the State promote dissent? Progressives have not dropped out of the system as have many libertarians, independents, and conservatives. I should have by now proven “Harm reduction” is the UN agenda. Carlyn attacks local governance and promotes the UN agenda as do most harm-reductionists, consciously or not. Modern progressives do not believe in freedom instead they believe in technocracy, they claim science as their guide but in practice it is a privileged class which interprets science and history according to their own ideological biases.
Just because I am against the States drug war does not mean I promote drug use. The dichotomy is easy to fall into because the state’s drug war has caused so much harm, most have no choice but to join progressives in opposing the State.
Both sides march blindly into technocracy, surveillance, and medical tyranny at an equal pace. The conservatives simply wish to expand the criminal powers of government. The libertarians are represented by the CATO institute and defend open borders and diminish the role illegal migrants play in drug trafficking, they also defend doctors against claims of over-prescribing. CATO blames US citizens for trafficking drugs across the border (but fails to mention they work for the cartels) while they condemn interventions against drug manufacturers in Mexico and lobby to remain soft on crime. But they also present valid data which defends harm-reduction strategies and why criminalization does not work.
As the world increasingly rejects Zionism for the genocide its producing in Gaza, conservatives are represented by hardliners that defend monopoly capitalism (claiming the yoke of “free-enterprise”) and militarization of local police. The deplorable conduct of establishment-conservatives taints Christians and conservative values and the American myth which includes meritocracy, equality under law, and self governance. But neither am I proud of rural America as they have allowed the destruction their culture; most are addicted to Marlboro, McDonalds , and Mountain Dew if not also gaming, gambling, and porn.
“The image of the morally upstanding peasant was invented only to be defeated, and the culture of the country-side was glorified only at the moment of its disappearance.” Surviving Capitalism Erik Ringmar
Tyranny is so bad progressives are defending our rights;
Like Justice Sotomayor in her dissent [Culley v. Marshall] for the three liberal justices, Gorsuch emphasizes the abusive practices of the modern asset forfeiture regime, and the fact that most of it is of relatively recent origin, arising from the growth of the War on Drugs. Supreme Court Issues Flawed Ruling in Asset Forfeiture Case, Ilya Somin, 5.9.2024, Reason
The RINO conservatives role is now to defend excess policing, asset forfeiture, and increased penalties to continue the war on drugs. Currently they are prosecuting users who sustain their drug habit by dealing as murderers. These charges include sharing (with or without commerce) tainted drugs with the legal presumption that the dealer knows the drugs are contaminated while the user is automatically absolved of the same expectation to know. It is convenient that the guilt is fully absolved of the deceased party, thus making them victims and martyrs and their families blood thirst justified. Characters in the movement, often whom admit the drug war was a failure, hold the correct concept that jail is necessary to combat the addiction; but they are too near sided to realize as they promote these increased penalties that there is a difference between charges which carry life sentences and a new jail/ drug court model. I am speaking of Ginny Burton and Sam Quinones; both promote increasing penalties, murder charges, as do hard line conservatives. Assuming a large gap between their philosophies it is not a stretch to assume many other informed activists hold this increased penalty [up to murder] position. Not me! I argue against the Left and the Right.
Sometimes called the “either-or” fallacy, a false dilemma is a logical fallacy that presents only two options or sides to an issue when there are actually more complexities.
*
State lawmakers consider harsher penalties for fentanyl possession, Nation, Mar 20, 2023:
Ingesting 2 milligrams of fentanyl can be fatal, meaning 1 gram — about the same as a paper clip — could contain 500 lethal doses.
Before this year’s legislative sessions began, a dozen states had already adopted fentanyl possession measures, according to tracking by the National Conference of State Legislatures. And in this year, in one legislative chamber of liberal Oregon and one chamber of conservative West Virginia, lawmakers have agreed upon tougher penalties.
In Nevada, where Democrats control the Legislature, a bill backed by Democratic Attorney General Aaron Ford would give one to 20 years in prison for selling, possessing, manufacturing or transporting 4 grams or more of fentanyl into the state, depending on the amount. It’s a change for Ford, who has supported criminal justice reforms including a sweeping 2019 law that, among other provisions, raised the threshold for such penalties to 100 grams. It would also remove fentanyl from the state’s “Good Samaritan” law, which exempts people from criminal drug possession charges while reporting an overdose.
Harm reduction advocates are pushing Ford and others to rethink their support, arguing the thresholds for longer penalties can sweep up low-level users — not just the dealers the law is aimed at — as well as some who may not even know they are taking fentanyl. They warn that the state’s crime labs test only for the presence of fentanyl, not the exact amount in a mixture of drugs. Thus, people with over 4 grams of drugs containing a few milligrams of fentanyl could be subject to trafficking penalties, they say. Rosa Johnson runs a needle exchange where she meets people who could face consequences should the stricter fentanyl bill pass. For the dozens of people that show up each day, it is rare for them to cite fentanyl as their “drug of choice.” But it’s also rare that fentanyl test strips come back negative, with the drug being “laced in a lot of things,” Johnson said.
“give me the man, and I will find the crime [for him]"
How Fentanyl is Leading to Murder Charges in California, BY THE LAW OFFICE OF CHRISTOPHER A. LAMIERO, March 15, 2021
Implied malice plays an important role in murder charges connected to fentanyl overdoses. Simply put, implied malice means a person knew their actions were harmful and potentially fatal, but decided to commit those acts regardless.
If you play any role ― major or minor ― in the sale or distribution of fentanyl, you could be looking at second-degree murder charges. This means that even if you, for example, transported the lethal drug in your vehicle or helped drug users find fentanyl dealers, authorities may charge you for murder AND drug crimes. Further, if you sell fentanyl-laced drugs to a friend who then sells it to someone else without your knowledge, you could be held responsible for that “someone’s” death even if you had no connection.
*
More Collar Counties charge dealers with drug-induced homicide for drug overdose deaths, ABC 7 Goudie, Markoff, Tressel, Weidner, Fagg, Aguilar
Leo Beletsky, a professor of Law and Health Sciences at Northeastern University, has been studying drug-induced homicide laws for years. "If you are responding to overdoses with drug induced homicide prosecutions, you're part of the problem, you're not part of the solution," said Beletsky. He said data doesn't support the theory that tough penalties stop people from selling drugs. Instead, he says, they criminalize vulnerable drug users such as family and friends rather than target drug distributors. Beletsky also claims threats of severe punishment cause fear among the drug-using population and that can result in fewer calls for help -- and more deaths.
*
Grothman, Banks Introduce The Stop Fentanyl Act, Washington, January 12, 2023 | Kyle Amato
“Currently, to trigger a 10-year mandatory minimum sentence under the Controlled Substances Act, an offense must involve 400 or more grams of a mixture or substance containing fentanyl. Because the average lethal dose of fentanyl is 2 milligrams, the offense would need to contain roughly 200,000 lethal doses in order to trigger the 10-year mandatory minimum.”
I hate to instantly jump to cynical conclusions; I have no way to interpret this double speak but as a belligerent intentional obfuscation and plain lie. As a press secretary for Mr. Grothman, Kyle should be clear and accurate. The initial sentence is simple “of a mixture or substance containing fentanyl” what follows is where the lie is embedded and glossed over “ lethal dose of fentanyl is 2 milligrams, the offense would need to contain roughly 200,000 lethal doses”. Lie! Excuse! Rhetoric! The most important question, the question the statement claims to address, is how much fentanyl triggers the penalty, not the weight of the baby laxative in the sample but the exact quantity of the fentanyl. But it gets worse:
Specifically, the bill:
-Amends the Controlled Substances Act and Controlled Substances Import and Export Act to reduce the 10-year mandatory minimum threshold for fentanyl offenses from 400 grams to 5 grams and fentanyl analogue offenses from 10 grams to 0.05 grams;
I allege 5 grams of baby laxative with .01mg of fentanyl will qualify you for their blood lust. Yes, it is true that analogues can be more powerful than fentanyl. Do you know if there is sodium chloride or potassium in your pickle juice? It’s even listed on the label but do you know? Or when you grab a pastry at the coffee shop do you know if they used butter or oil? Of course you don’t! Anyone in possession of any substance weighing .05 grams containing any detectable trace of a fentanyl analog will go to prison. If the term without that individual’s knowledge is included in law I presume it will be fully ignored during prosecution because this term alone nullifies the entire law, who knows how much or even if any fentanyl is in counterfeit pills. If phone records indicate the accused is asking for blues or 30’s or bars how can the state infer that they did or didn’t want fentanyl.
-reduce the 5-year mandatory minimum threshold for fentanyl offenses from 40 grams to 0.5 grams and fentanyl analogue offenses from 10 grams to 0.005 grams;
It’s clear we are playing the measurement game again. What these tiny measurements mean is simply possession of even one pill can put you in prison for 5 plus years and maybe even qualify for murder charges. Are we going to be using PCR tests to check weed for fentanyl on the side of the road? If you thought you bought a Xanax or Adderall and it’s dirty you will be charged for the weight of that pill as if it’s pure fentanyl. This is what I believe based on the lack of clarity, a lie by omission. I challenge you to ask how the contents of these pills will be tested, isolated in a lab or will it be the plea-bargain that determines guilt?
Murder
Children who share pills get prosecuted for Murder while others are too rich to jail:
Warnock delivered a speech expressing concerns about the bill as drafted, arguing that it “will make life safer for bankers for businesses and financial institutions, some of whom have been profiting from the cannabis industry illegally for years.”.S. Senate Committee Approves Bipartisan Marijuana Banking Bill, Sending It To The Floor September 27, 2023, By Kyle Jaeger
Inherent in using (even unadulterated) Fentanyl is a potential to kill, specifically with an inaccurate dosage, and a high probability for addiction. A fundamental question is if the law can determine that informed consent was present during acquisition and self administration of Fentanyl. We all know the prison military complex will prosecute and railroad anyone too poor to fight back and those with power and status will avoid accountability.
Bereaved parents march for blood. Although hard to accept; their children chose to do illegal drugs knowing the broad range of inherent risks. Most overdoses are caused by mixing drugs, (poly substance) which places overdose within the users control, of course the quantity the “victim” consumed is also within their control. Whether or not they know the purity of the contents they chose how much of those contents to administer (usually with the knowledge that they do not know the purity of the contents).
(billthatwouldiowa)
(idaho 406)
“Yet this attitude belies a fundamental misunderstanding of the situation, considering that many addicted users become dealers simply to support their habits. “These aren’t two distinct sets of people,” said Maryland public defender Kelly Casper.” They want to charge all of these people with drug dealing, when in fact the core of the problem is that they’re users.” FI 237
Bereaved parents deceased children could have shared their contaminated drugs with friends. They would then be subject to the same murder charges, instantly converting them from victims to offenders. I assume these same parents would march for lesser penalties if their children were in prison for murder for sharing a dirty Adderall they bought on Tik Tok. Are users innocent if they didn’t know it was fentanyl? Aren’t they guilty of illicit drug use? Is ignorance of adulterants an excuse when buying random drugs from an untrusted source? Does buying dirty drugs make you innocent?
Many conservatives and disgruntled parents rally for blood. They want dealers locked away with mandatory minimums, lower thresholds (as little as two pills may qualify you as a dealer), and even for missiles to be dropped on Mexico. These hot heads believe granting the govt latitude is going to protect their children who are at an age of rebellion and experimentation. Many users are small scale dealers just earning enough to stay “well”. I would argue dealing is also more honorable than “boosting”, violence, or sex work. Both parties voluntarily contracting on equal footing (small scale dealers/users). Nobody is claiming the seller is also the manufacturer and so its obvious (“a reasonable doubt”) the seller does not know exactly what they are selling.
Murder
“Buyer Beware” is a maxim for a reason. By now, purchasers of these drugs know there is no guarantee of safety or purity when they buy from the black market and their never was a guarantee. Buying weed in my youth I would drive to some ally in the ghetto and hope for the best. It is delusional to believe your child was so innocent and naive not to be expected to understand that illicit drug use carries severe risks. And worse is if they want fentanyl by name, as established addicts do. There is no way to definitively prove what a buyer knows or expects or how far along in addiction they are; some alcoholics drink rubbing alcohol. Conservatives seeking life and death sentences for “dealers” rely on unfounded speculation that all “dealers” know their supply is dirty and conversely that all users are innocent and do not expect any contamination of their drugs, although dirty drugs have been the norm for decades. Every cocaine user knows their drugs are diluted. Lawmakers claim that users don’t originally desire fentanyl and that may be the case at the beginning of the addiction but once addicted the user obviously knows and expects it. Is it poisoning if the buyer knows that it is poison, who pulls the trigger in a suicide? Are we playing 9 ball? Are we placing all the blame on the last straw that broke the camels back?
Volkow provides valid reasons why we can’t charge dealers with murder. I agree despite my opposition to her. Volkow did not intend my point by her statement below but she would none the less oppose harsh penalties for addicts;
“Several identifiable characteristics among patients have been reliably associated with an elevated risk of opioid overdose. Included among these factors are a history of overdose, a history of addiction to any substance (but particularly alcohol, benzodiazepines, or opioids), and health problems associated with respiratory depression or concurrent prescription of any medication that has a depressive effect on the respiratory system, such as benzodiazepines and sedative hypnotics. The presence of renal or hepatic dysfunction also increases the risk of overdose, since in patients with either of these conditions, the clearance of many opioid drugs is impaired, which leads to higher and longer-lasting drug levels in blood. Finally, because some cases of overdose may be purposeful suicide attempts, a history of suicidal thoughts or attempts and a diagnosis of major depression are also markers for an elevated risk of overdose. Opioid Abuse in Chronic Pain — Misconceptions and Mitigation Strategies, Volkow, McLellan, March 31, 2016
Life and death sentences also endanger cops; criminals are already belligerent, paranoid, and defensive, once they literally have everything to lose with harsh sentencing they will have nothing to loose and may resort to violence to avoid being taken in knowing they’re already at their end.
Conclusion
Your duty is in protecting yourself and your family from succumbing to this snare. Growing up, I’ve seen many elders illegally using prescription opioids. Does this mean doctors are harbingers of morality? No, but this reality should alert you of the current dangers of look-alike pills containing fentanyl. And for the youth, experimenting is more dangerous than ever as most black market drugs are deadly dirty. Besides, ecstasy often leads to meth! Children prescribed Adderall today, and many more without prescriptions who abuse the stimulant may later look to the black market.
Worse, when public outcry forces the State to reel in Adderall and Xanax prescribing later it will create a void to be filled with dirty black market substitutes. I expect a ridiculous explosion of fentanyl addiction (and deaths) as a result of this. Meanwhile it gets worse everyday for many reasons, not least of which is mass despondency. We have not registered the severity of this yet. Keeping the reality of this epidemic, and the subversive goals of harm-reduction, swept under the rug is not going to aid in our understanding when this takes over the news. This is the a pandemic! When this finally gets the attention it deserves the Regime will have some tyrannical solution it is selling us. “challenges include difficulty of convincing people to take medicine when they are not sick.” AF 150
I don’t respect “toxic individualism” or excessive self-seeking which is the basis of our legal-economic model [late stage capitalism, state-sponsored usury]. I blame this Americanism for my own broken family. Besides arguing these larger issues my point is that I am not doing this work for most users. I am doing it for the few who are fighting to better themselves and fighting to keep these drugs and needles (and their de-stigmatization) away from innocent children (and those adults among us who can’t govern themselves). Even if I don’t directly reach them, I reached you and imparted valid criticisms and useful tools.
What motivates me to work in this topic is the lack of public awareness. I am aware of many theories regarding our dystopian future but in most cases there is little I can do to change it. I can spend my efforts arguing against technology and convincing you to remove surveillance devices from your home but we can’t run or hide anymore. In my opinion politics is beyond reform. I am an anti-federalist but I will be the first to criticize Jefferson as a radical liberal. Preserving useful remnants of our culture is still possible. Dr. E. Michael Jones’s writings have been exposing psychological warfare and promoting freedom from the bondage of pornography and drugs for decades. It is from this background that I defend regulating drugs as opposed to the “free market-voluntarist- libertarian, anarcho-capitalist” perspective. No one should easily dismiss the amount of research and dedication I have invested to come to my opinion on Fentanyl or the law. If a citizen can not exercise self-governance why shouldn’t the state assume the responsibility. In my first letter on weed I supported Judge Napolotanos position which is decriminalization instead of legalization. Napalatano’s position still best describes me but Fentanyl is different. America’s lack of leadership from within the family or by the community leaves no choice but for incarceration. It should be clear by now I have no faith in the State either.
If I had to chose one solution besides a new jail model (that likely won’t happen on a meaningful scale) I would jail addicts and medically treat them for a 3-7 day detox and then impose onto them extended release buprenorphine (Sublocade), or prior to induction to buprenorphine and after detox, they can make the choice to get abstinent via extended release Nalrexone. I would tether them somehow to ensure they return for their next monthly dosage. Buprenorphine carrying with it the expectation to taper off (90 pages to explain why). There’s my simple evidence informed approach.
If rights and freedom of choice are a question then I believe the other choice offered should be longer incarceration because street-fentanyl addicts (not all addicts) are a danger to themselves. I think 6 months of a new jail model is the minimal that would be needed.
Solutions
“A “failure” of addiction treatment all too often leaves the patient dead. It is high time we put the responsibility where it belongs OO 242
Drug use is wrong but tough love may not be right course;
“So called tough love, Schultz says, alienated people who use drugs without either dealing with the reasons they use, or providing help with the withdrawal and cravings that so frequently lead people pushed into abstinence back to the drugs, and to fatal relapse, with no further chances.” OO 103
A slightly different approach would give far greater credit to poor people who use drugs for the survival skills. For balancing the pursuit of security and the pursuit of autonomy in the most difficult of circumstances. Existing healthcare, addiction treatment, and social service systems all put up barrier after barrier to them. These range from smoking bans for people who are now asked to withdraw from heroin or illicit fentanyl and nicotine simultaneously, to barring family from rehab or withholding contact for minor rule infractions. All for no reason except, it seems, to humiliate and remind people that “once a junkie, always a junkie”- that is, that by being poor and having used opioids, you have forfeited basic rights such as being treated with the respect we accord to other human beings. OO 166
“today only one in six patients with an addiction seeks treatment.” AF 84
I would add that couples, nor families or pets should have to separate perhaps any longer than for sleeping arrangements. These dehumanizing stipulations make it harder for those who otherwise would seek help.
“To get the medication that keeps him well, Joe must travel to a distant Toronto suburb, where his methadone clinic is hidden behind an auto body shop. By the time he arrives there in the morning to stand in line or squeeze into the little waiting area, he is in serious withdrawal, sweating and shaking. Every week, he must provide urine samples. Joe sends me photos that he took from inside the bathroom where he must pee in a cup (in the US, this process often involves observed screening). Although at least he is allowed to lock the door, there are four cameras, some fixed at groin level to ensure he does exactly what he’s told.
The writer Elizabeth Brico, in Florida, experiences a similarly dehumanizing process when she undergoes witnessed urine drug screening as a requirement for receiving buprenprphine, one of the two most evidence-based treatments for opioid use disorder: “She watched, annoyed, while I pulled up my panties, tugged down my skirt, and sidled past her out the bathroom, empty cup in hand.”
Ultimately Brico relapsed with heroin as a result of her inability to pee under scrutiny.
Although some clinicians claim there is a safety value to patients in knowing what’s in their urine, the tests are notoriously unreliable and easy to mess with despite the punitive precautions, and there is no evidence that they improve patient care in any way. They allow doctors (even in single-payer-healthcare Canada) and laboratories to bill, often exorbitantly, for provision of the test, and in fact constitute an entire industry devoted to surveillance and reporting of the contents of the people’s piss and marketing of ever-more-creative ways to monitor human fluids. These include new, privacy-shredding ventures such as apps that allow for observed, recorded alcohol and drug screening.
Philadelphia harm reduction advocate Bill Kinkle, a former nurse who was addicted to heroin, also describes the trauma of this dehumanizing practice, in which he has regularly been forced to relive the helplessness of past sexual trauma and incarceration, including being raped in prison, as part of mandated addiction treatment. Never, he says, has his urine screening been witnessed by an observer of the same sex. He wrote to his case manager under Pennsylvania’s nurse monitoring program,
“I want to be as clear as possible here so there is no confusion. What happens every time I am selected for a screen is intense anxiety, cold sweats, and overall psychological heaviness. While I am preparing to go into the restroom I begin to shake and sweat more, most times I joke with the staff to cover the growing impulse to cry and leave the facility, while in the restroom I can smell the jail cell the night I was raped. I can feel the texture of the wool blanket over my face and hear the muffling of sound. My heart races, my voice cracks, and I have to work extraordinarily hard not to spill the specimen as I hand it over because I shake so profusely.” OO 177-178
Exceptions should not guide policy:
“Matt last injected heroin last week: he is, in fact, an occasional, recreational heroin user.. [he] practices a way of using heroin that was popular during the 1950’s, called “chipping”, where you take great care to avoid acquiring physical dependence by spacing out what De Quincey, who initially practiced this a hundred years avant la lettre, would have called his “debaches” and what Matt calls holiday, recreation like any other form of recreation.” OO 262
“Remission may not always require abstinence, for instance in the case of alcohol addiction, but is a reasonable proxy for remission with opioids, where return to controlled use is rare.” Neuropsychopharmacology 46 Addiction as a brain disease...
The Sinclair method is one such technique which doesn’t adhere strictly to abstinence but promotes moderation as a more realistic goal (for alcohol). And I agree there should be as many options or tools available as possible for those seeking to better themselves. I remind readers Fentanyl is much more powerful; if we are gathering data from from self-reporting I don’t believe we can trust addicts to be honest about their drug use.
“Indeed cannabis is a very promising alternative or adjunct to lower doses of opioids or other drugs- but it’s long- term effects are largely unknown, and its effect on cognition and motor skills means that it is definitely not a good option for all pain patients, even when it does work to reduce the perception of pain.” OO58
My list would look more like
1. Prevent initial drug use, keep kids busy and sheltered
2. Involve parents and promote private local organizations, provide opportunities
3. Beware of social media, regulate advertisers
4. Prevent over prescribing of Adderall and Xanax, etc.
5. Instead of restricting access to RX opioids make them available for those who need them
6. Public campaigns and free Naloxone and kratom for OUD, alcoholism, and overeating
7. Lower barriers for riskier detox drugs; gabapentin and Suboxone but retain professional oversight
8. Safe comfortable detox sites, new jail model
9. Stigmatize all drug use, including process addictions, campaign to promote clean sober living
10. Provide a society that people don’t need drugs to cope in, containing hope for the future
11. Incentivize work and sobriety
Carlyn discovered and uses mindfulness-based stress reduction (MBSR) developed by Jon Kabat-Zinn. “The approach is based on buddhist principles, with the mysticism stripped out. MBSR training, sometimes combined with cognitive-behavioral psychotherapy, is now widely offered across North America for the treatment of chronic pain, anxiety, depression, and a host of other conditions. Despite practicing mindfulness, however, I find that it remains extremely hard to prevent ongoing pain from veering into complete despair… Opioids replace the non-judgment of mindfulness with a powerful attraction to what feels good. Despite the sinful connotations of pleasure-seeking, that attractive sensation of calm observation- Rebecca Solnit’s reptilian feeling- is the same empty, comfortable detachment that the experienced mediator may occasionally feel. It’s equally analogous to the notion of “flow”...” OO 57
“, mindfulness is one the newer and most prominent strategies for dealing with addition and its siblings. In all cases, the issue is one of unbearable sensation…. The remedy for sensations of awfulness that the human psyche is not well equipped to handle is detached, curious, calm, and focused observation. It’s an attitude easily reached while under the influence of opioids, but one that takes hard daily practice- hourly or constant practice, even- without chemical help.” OO 67
ACT (Acceptance and Commitment Therapy) OO 258
These are some drugs that may help detox:
Clonidine or Lofexidine helps with body sweats crawling skin, redcues blood pressure
Buspirone or benzodiazapine helps with anxiety
Trazodone helps with sleep; usually very easy to get some from a doctor
Ondansetron helps with nausea
Imodium helps with diarrhea
supplements:
and Sodium Ascorbate (buffered vitamin C to avoid hyperacidity issues
DLPA (DL-Phenylalanine) helps with depression, chronic pain and neruotransmitter support
GABA promotes relaxation and eases nervous tension
5-HTP helps raise serotonin levels in the brain which may have a positive effect on sleep , mood, anxiety, appertite, and pain sensation
B complex, Ashwaganda
How to Detox from Fentanyl at Home, Katy, 12/10/2023
Factoids
“Many patients have more trouble stopping their use of a benzo like valium or Xanax than they do stopping their use heroin.” AF 41
These drugs may not have steep overdose deaths like fentanyl but may be more addicting and detox even be more dangerous . Keep in mind many drug abusers may be (legally or not) using benzos as well as fentanyl. Benzos are also increasingly found street pills mixed with fentanyl adding seizures to the list of possible dangers.
“patients receiving benzos and opioids were ten times more likely to overdose than those receiving opioids alone.” AF 162
Benzodiazepine and opioids can be an especially deadly combination, since both drugs slow down the central nervous system, which affects breathing. Indeed, the NIDA says that more than 30 percent of overdoses involving opioids also involve benzodiazepines… We have this whole infrastructure set up now to prevent overprescribing of opioids and address the need for addiction treatment,… We need to start making benzos part of that.” Dr. Anna Lembke, Stanford, FI 276
Other procedural solutions being proposed, debated, and implemented; testing everyone for fentanyl in emergency rooms, opposition says its a waste of resources and not even possible. Same criticisms for full autopsy vs toxicology for all deceased.
Sleep through withdrawals, YouTube channel Advanced Rapid Detox is a technique where they drug you into a coma for the duration of detox. I believe in Justice for those who do wrong (and drug abuse is wrong) and for many that justice will be the severity of withdrawal and the pain of rebuilding the life they destroyed. But my intentions are not driven by blood lust and I am not the Creator. If this technique works I endorse it. Yes, the pain makes us grow but I am not like the Amish at the dentist who refuse analgesics either.
A personal testimony
“Yeah that's interesting and alarming to think that it's going to get worse. I wonder how far it can get. I think that kratom is probably the best option for quitting but it's not simple. Someone has to truly be ready to quit and they probably should already have a taper plan laid out. Also some sort of counseling is needed. Maybe not "therapy", but it would help to talk to someone who has some sort of training and lots of knowledge. I'm not sure how I feel about Suboxone. It definitely saved my life but I've been on it for way too long. Kratom is much easier to quit. Withdrawal is way less harsh. Suboxone withdrawal can last up to a month and the post acute withdrawal syndrome can last like 6 months! Much worse than heroin. Not as bad as methadone. I'm not too familiar with fentanyl withdrawal but I would imagine it's fairly short and intense. I'm finally on my last few months of tapering Suboxone and I’m stoked but also afraid of the impending post acute withdrawal. Although it's not uncommon for it to take some people 10 or 20 years or sometimes the rest of their life, I think part of the reason it's taken me so long is because for the majority of my time on Suboxone I sourced it myself and didn't have a doctor. I've actually only had a doctor about 2 years ago and I was going there for about a year. They prescribed me way more Suboxone than I actually need so I just saved it up and stopped going because I had to go there once a week and it was an hour drive from my house. So I saved up and came up with a plan on my own, but that's really not a very good idea I would guess. Before getting the doctor, I would have to buy them for sometimes $20 each. I'm glad I don't have that expense any more!”
I don’t have much to follow that I haven’t already written. I am not sure if withdrawal from fentanyl is any shorter because it is fat soluble (lipophillic) so it stays in tissue longer. Keeping in mind my lack of scientific understanding I will venture to add that buprenophrine has a long half life which may not aid in withdrawal. I am proud of him because he wants to quit, he is finding a way with any tools at this disposal. I hope he appreciates my efforts here.
Mexico Case
Now that you fully understand the basis for opposition to harm-reduction tenets, you are ready to dissect Mexico’s position. I will add despite fan fare for the new president and my limited knowledge of Mexican politics I do know something about ideology and harm-reduction specifically. I allege the new president will gleefully adopt harm-reduction policies while the previous president strongly opposed them:
“Second, the current administration's approach to substance use has been from a moral rather than a public health perspective. For example, the main strategy for substance use prevention under the current administration is that of anti-drug public service announcements. This media campaign launched by the National Addiction Prevention Strategy first used the slogan “There is no happy ending in the world of drugs”, later changed it to “The world of drugs is not a happy place” and finally “If you do drugs, you hurt yourself”. Among other things, some of these campaigns further suggest that most people who use drugs (PWUD) do so because they are not happy, and the president has publicly called for the stigmatization of substance use.
“Historical lessons from 100 years of drug education in the US have shown that these types of messages, which convey strict abstinence, are not as effective in reducing substance use when compared to messages that encourage informed choice from a harm-reduction perspective.”
“Poverty and drug-related violence have also fueled the proliferation of informal and coercive centres for substance use-disorder in the country that exacerbate the suffering of its residents through forceful rehabilitation techniques. The majority of people who receive treatment in Mexico do so at abstinence based residential facilities”
“Research including data from Mexico shows that people who undergo coercive drug treatment are more likely to suffer a non-fatal overdose than people who do not. Therefore, PWUD are exposed to higher overdose risk when they are released from these types of drug treatment facilities in Mexico.”
Drug treatment policy in Mexico is certainly not modern. Methadone is limited, Suboxone and naltrexone are not available, and buprenorphine is only prescribed as a treatment for pain. The abstinence model is arguably primitive and even punitive not only because the pain of withdrawal but also because risk of overdose upon release is a real danger (termed death-by-rehab). But because of the barbarity of their policy it leaves an opportunity for valid criticism. Viewing this article in its entirely demonstrates how defending Narcan is the thin of the wedge.
“Implement a free national low-barrier opioid treatment scheme with medications such as methadone or buprenorphine.”
“the Mexican President declared that naloxone “prolongs the agony of people”.
I understand his position (throw good money after bad). When we debate on how to use public funds why should those who are so far down the path of self-destruction and addiction receive benefits? How much prevention could that money buy instead? But taking a stern conservative position on the issue with no room for nuance fuels back lash.
Harm-reduction advocates don’t just want nalrexone or MAT;
“Even if this minimal and simplistic legislation passes during the current, or in an incoming administration in 2024, there is a risk that no further meaningful action related to opioid overdose prevention occurs. This may lead to the unintended consequence of extinguishing the sense of urgency in addressing opioid overdose at the national level. Since the government has no program to assume the financial costs of naloxone distribution, these costs will be transferred to people who use opioids, their families, or community organizations that are already doing the work on a voluntary basis through donations.”
“Key issues in the effort to reduce opioid overdoses include the distribution of naloxone at the community level, making the medication affordable for harm reduction efforts, or the establishment of an organization to develop meaningful lines of action”
This is about establishing and funding this “organization”. This organization will exist to adopt the entire woke agenda.
but are not limited to: 1) create mechanisms and materials for recording overdoses in community settings, forensic medical services,
this is burdensome and the US is still having difficulty implementing this.
“design evidence-based campaigns and training on substance use treatment and opioid
overdose care with naloxone such as talks and workshops...to sensitize them on public health issues…”
It begins:
“implement a free national opioid treatment scheme with medications such as methadone or buprenorphine, substance testing, syringe exchange, and overdose prevention rooms”
To date, the government has turned its back on reducing harms by defunding harm reduction organizations that provide sterile syringes or HIV screening and prevention”
The reason this is such a great case study is in how it presented. Very little is discussed about the later steps and their validity. The “woke” advocates rightly defend saving their lives with Naltrexone and helping them recover with MAT but shortly they will push for needle exchanges and drug testing as those are also valid and less controversial. Once the money, authority, and framework are established those same entities will have no choice but to adopt and pursue what follows. What comes next is alluded to if you know what your looking at but otherwise strategically left unsaid.
JASL was supported by the Canada Research Chairs Program. DGM was supported by the US National Institute on Drug Abuse.
This is a case and point of how political subversion by the Regime is rolled out.
Implementing a decentralized opioid overdose prevention strategy in Mexico, a pending public policy issue, Lancet Reg Health Am, 2023 Jun 17
FI FENTANYL, INC., Ben Westhoff
BP BITTER PILLS, Stephen Fried
on OPIUM, Carlyn Zwarenstein
AO AMERICAN OVERDOSE, Chris McGreal
AF THE AGE OF FENTANYL, Brodie Ramin, M.D.
Hi Matt... I stumbled into your substack, probably looking for another Matt. I stuck around cause I saw you write on an EGLE meeting and liked your speech... and then I came across this long gem.
To be honest, i cannot manage to read this whole document in one sitting. I managed about a quarter and will get back to it this weekend.
However, I want to tell you to keep it up. You are a great researcher, and have an incredible command of many things. I particularly appreciate your direct language which is in sharp contrast to fluff all around us.
Also the subject matter is really relevant to the time we live in, where more and more of us will follow the coal miners or are already well versed in the knowledge of an addiction.
PS (I live in michigan and my father in law was probably one of the older dudes you mentioned at egle, though I am much more aligned with your perspective).